Laparoscopic Low Anterior and Abdominoperineal Resection
Virginia Oliva Shaffer
Steven D. Wexner
Indications for laparoscopic colorectal surgery do not differ from those for open procedures except for the method of access. As in open procedures, laparoscopic abdominoperineal resection is appropriate only for carcinomas that invade the anal sphincter or that cannot be curatively resected with an oncologically acceptable distal margin. Laparoscopic low anterior resection is appropriate for cancers in the mid (5 to 10 cm from the dentate line) or distal rectum (less than 5 cm from the dentate line); in these cases, a total mesorectal excision (TME) with a coloanal anastomosis should be performed.
Preoperative evaluation, mechanical and antibiotic bowel preparation, and thromboembolic prophylaxis are also identical to those measures employed for open procedures. Preoperatively, an enterostomal therapist selects and marks the preferred site for a temporary or permanent stoma.
In this chapter, we describe both laparoscopic low anterior resection and laparoscopic abdominoperineal resection; performance of the coloanal anastomosis as the intra-abdominal component of the procedure is identical in both settings. Regardless of the procedure and technique, performance of a TME is of paramount importance in the cure of tumors in the lower two-thirds of the rectum. Included with the TME are oncologically acceptable radial and distal margins and adequate lymph node harvest.
SCORE™, the Surgical Council on Resident Education, has not classified laparoscopic low anterior and abdominoperineal resections.
STEPS IN PROCEDURE
Modified lithotomy position
Umbilical trocar site; thorough exploration of abdomen
Additional trocar sites: Right lower quadrant, right paraumbilical, left paraumbilical, or right upper quadrant
Steep Trendelenburg position with table tilted to the right
Grasp sigmoid colon and retract medially
Incise line of Toldt and mobilize colon medially
Identify and protect ureter
Mobilize splenic flexure without pulling on spleen
Divide inferior mesenteric vessels
Elevate uterus and adnexa in female
Grasp rectum and retract cephalad and anteriorly
Incise peritoneum laterally and anteriorly
Dissect in avascular plane along iliac vessels (preserving ureters) and presacral space
Anteriorly, the plane should be just deep to vaginal wall (female) or seminal vesicles (male)
For Low Anterior Resection, Divide Rectum at Chosen Point with Linear Stapler
Lengthen infraumbilical trocar site to 3 to 5 cm, place plastic sleeve, and remove specimen
Create J-pouch with linear stapler
Return colon to abdomen and close incision, re-establish pneumoperitoneum
Create stapled anastomosis with circular stapler, inserted transanally
Create loop ileostomy
Close trocar sites in usual fashion
For Abdominoperitoneal Resection
Complete mobilization of rectum to levator muscle
Perineal phase of operation is performed as usual as a cylindrical excision
Remove specimen through perineal wound
Create end colostomy
Place drain
Close trocar sites in usual fashion
HALLMARK ANATOMIC COMPLICATIONS
Injury to ureters
Injury to spleen
Bleeding from presacral venous plexus (improper dissection plane)
Laparoscopic Low Anterior Resection
Preoperative Setup and Trocar Placement (Fig. 102.1)
Technical Points
Place the patient in a modified lithotomy position with the hips and knees gently flexed at a maximum 15-degree angle. Greater elevation of the thighs may not allow the surgeon to freely move the instruments. The buttocks should slightly extend over the end of the operating table. This position gives proper access to the anus for endoscopy and for insertion of a circular anastomotic device and also allows access to the perineal region for abdominoperineal resection. Both arms are tucked at the patient’s side and must be carefully padded to help avoid ulnar or brachial plexus injury. The patient must be safely secured to the bed by either taping, use of beanbag, or shoulder restraints. A monitor is placed on each side of the patient. Bilateral ureteral stents are placed by a urologist at the discretion of the surgeon. A warm-air, upper-body warmer across the chest and above the nipple line is used to help avoid hypothermia. Place an orogastric tube and a urinary catheter to minimize the risk for gastric or bladder injury, respectively, during trocar insertion. Prepare and drape the abdomen and perineal region for a laparotomy in case a laparoscopic procedure cannot be completed. The surgeon stands on the right side of the patient, the first assistant surgeon on the left, and the second assistant, who controls the camera, to the left of the surgeon.
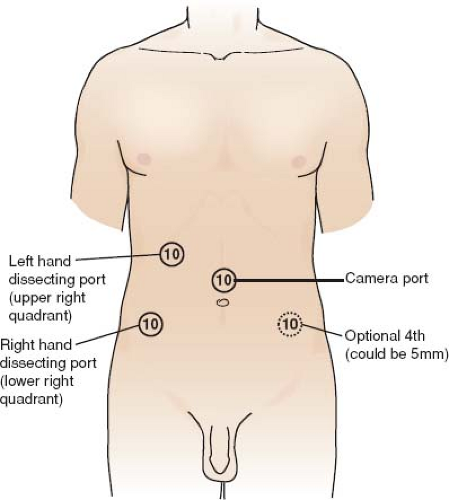 Figure 102.1 Preoperative setup and trocar placement |
A CO2 pneumoperitoneum of 12 to 15 mm Hg is established in the usual fashion, through a small vertical infraumbilical incision. A 30-degree laparoscope is then introduced, and the abdomen is thoroughly explored to assess other pathology and to determine any metastatic dissemination. To inspect the liver, the patient is brought into a steep reverse Trendelenburg position; if desired, a laparoscopic ultrasound of the liver may be performed.
If the proposed operation is deemed feasible, the other ports will be positioned. The operation is facilitated by the camera and the instruments being interchangeable to all ports. The 10-mm bipolar energy device is preferred for division of the inferior mesenteric artery and vein. Accordingly, only 10- to 12-mm trocars are used; three operating port sites are usually sufficient. Place the additional trocars under direct laparoscopic visualization in the right lower quadrant and in the right upper quadrant in the midclavicular line. The port positioning takes into account the patient’s anatomy, the location of the incision for specimen retrieval, and the site of any planned stoma. An optional fourth 10-mm port may be placed in the left lower quadrant to help mobilize the splenic flexure in tall patients, retract the small bowel in obese patients, and retract the uterus in women with a large uterus. This optional port may also be useful for retraction of the prostate and seminal vesicles in men with a narrow pelvis.
The following additional instruments are required.
Four 10- to 12-mm trocars with reducer caps
Ultrasonic scalpel or harmonic scalpel
One 10-mm bowel clamp
Two 10-mm Babcock graspers or atraumatic bowel graspers
Both 30- and 45-mm endoscopic linear cutting staplers
A 29- or 33-mm endoscopic curved intraluminal stapler
A 75-mm linear cutting stapler
A 5-inch plastic wound protector
Mobilizing the Sigmoid and Descending Colon (Fig. 102.2)
Identification and Preservation of the Left Ureter (Fig. 102.3A, B)
Technical Points
Place the patient in a steep Trendelenburg position with the table tilted to the right side so that the small bowel gravitates toward the right upper quadrant of the abdomen and no retraction to the small bowel is required. Gently grasp the sigmoid colon
with a Babcock clamp or atraumatic bowel grasper through the right paraumbilical port, and move the bowel to the patient’s right side. This maneuver places traction on the posterior peritoneum overlying the iliac vessels. Incise the peritoneum with the ultrasonic scalpel, harmonic scalpel, or shears with cautery placed through the right lower quadrant port. Sequentially slide the device under the peritoneum, and advance it down the pelvic sidewall toward the anterior peritoneal reflection, using it to push the mesorectum and mesosigmoid medially away from retroperitoneal structures. Identify the ureter as it crosses the iliac vessels and trace it proximally as far as possible.
with a Babcock clamp or atraumatic bowel grasper through the right paraumbilical port, and move the bowel to the patient’s right side. This maneuver places traction on the posterior peritoneum overlying the iliac vessels. Incise the peritoneum with the ultrasonic scalpel, harmonic scalpel, or shears with cautery placed through the right lower quadrant port. Sequentially slide the device under the peritoneum, and advance it down the pelvic sidewall toward the anterior peritoneal reflection, using it to push the mesorectum and mesosigmoid medially away from retroperitoneal structures. Identify the ureter as it crosses the iliac vessels and trace it proximally as far as possible.
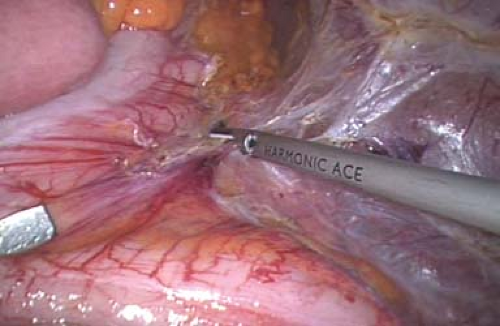 Figure 102.2 Mobilization of the sigmoid and descending colon |
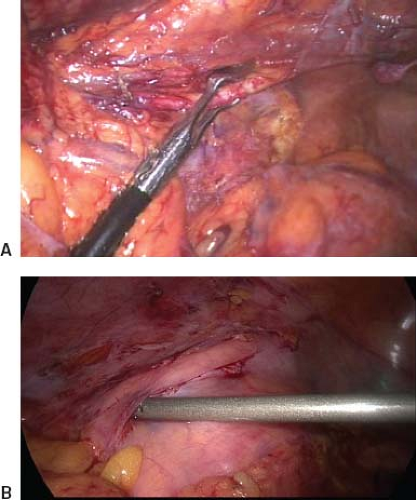 Figure 102.3 A: Identification. B: Preservation of left ureter. |
Anatomic Points
The abdominal and pelvic part of the ureter lies in extraperitoneal areolar tissue. The abdominal part, which descends on the medial part of the psoas major muscle, enters the lesser pelvis anterior to the end of the common iliac vessels or the beginning of the external iliac vessels. The left ureter lies beneath the root of the sigmoid mesocolon. The right ureter lies behind the lower part of the mesentery and the terminal ileum. In the pelvis, the ureter is anterior to the internal iliac artery and is covered by the parietal endopelvic fascia. Laterally, it lies on the fascia of the musculus obturator internus. In males, the ureters pass between the internal iliac vessels and the ascending vas deferens. Then they turn anteriorly, pass along the levator ani, and penetrate the base of the bladder in front of the seminal vesicles. In females, the pelvic part at first has the same relations as in males, but anterior to the ureters lie the ovaries. At the pelvic floor, the ureter turns anteriorly on the levator ani, turns forward slightly above the lateral vaginal fornix, and then inclines medially to reach the bladder.
Mobilizing the Splenic Flexure (Fig. 102.4A, B)
Technical Points
Place the patient in a steep reverse Trendelenburg position. This position allows the transverse colon and viscera to fall away from the spleen and the stomach. While the assistant retracts
the splenic flexure toward the umbilicus with the Babcock clamp, separate the mesentery of the descending colon from Gerota fascia until the splenic flexure is reached.
the splenic flexure toward the umbilicus with the Babcock clamp, separate the mesentery of the descending colon from Gerota fascia until the splenic flexure is reached.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


