Laparoscopic Gastrostomy and Jejunostomy
These procedures are useful either as incidental procedures during other laparoscopic operations (e.g., gastrostomy performed in association with laparoscopic repair of paraesophageal hernia) or when other methods of access fail. The stapled Janeway gastrostomy, shown here, can also be done as an open procedure when a permanent gastrostomy is desired. The mucosa-lined tube that is formed will remain patent without a catheter and can be covered with a simple dressing when not in use.
SCORE™, the Surgical Council on Resident Education, classified laparoscopic feeding jejunostomy as an “ESSENTIAL COMMON” procedure.
STEPS IN PROCEDURE—LAPAROSCOPIC GASTROSTOMY
Obtain laparoscopic access and choose skin entry site in left upper quadrant
Simple Gastrostomy
Make 1-cm long skin incision at entry site
Pass needle through incision and into stomach, insufflating air to confirm intraluminal access
Use Seldinger technique to pass guidewire and then dilator and sheath
Pass small diameter Foley catheter through sheath
Use T-fasteners to secure stomach to anterior abdominal wall
Secure catheter, close trocar sites larger than 5 mm in diameter
Janeway Gastrostomy
Place 12-mm trocar in right upper quadrant site, grasp stomach with endoscopic Babcock
Pass endoscopic linear cutting stapler through 12-mm port in right upper quadrant and use it to create a tongue of stomach
Pull the tip of the tongue of stomach up into the left upper quadrant trocar and withdraw trocar and stomach
Cut off the tip of the tongue of stomach and mature the mucosa to the skin
Cannulate
Secure catheter and close trocar sites greater than 5 mm
LIST OF STRUCTURES
Stomach
Pylorus
Suspensory ligament of duodenum (ligament of Treitz)
Jejunum
Laparoscopic Simple Gastrostomy (Fig. 58.1)
Technical and Anatomic Points
Obtain access through an infraumbilical incision. Identify the stomach. Place a second trocar through a right upper quadrant site (Fig. 58.1A) and insert an atraumatic grasper. Grasp the stomach and manipulate it until a suitable site high on the fundus is located. Confirm that it will pass easily to the underside of the anterior abdominal wall at the chosen location.
HALLMARK ANATOMIC COMPLICATIONS—LAPAROSCOPIC GASTROSTOMY
Injury to bowel or viscera
Submucosal (rather than intraluminal) passage of gastrostomy tube
Janeway gastrostomy—leakage from staple line
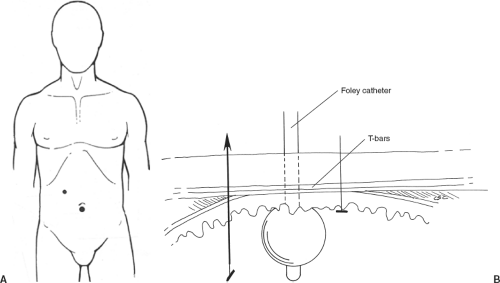 Figure 58.1 Laparoscopic simple gastrostomy |
Make an about 1-cm skin incision at the proposed site. Through the skin incision, insert a 14-gauge needle. Under direct visualization, puncture the stomach with the needle at the chosen location. Use the grasper to stabilize the stomach, facilitating puncture. Confirm that the needle is in the stomach by injecting and aspirating air or saline. Pass a guidewire into the stomach. Using a Seldinger technique, follow the guidewire with a dilator and finally a sheath through which an 18-French gastrostomy tube (commonly called a Foley catheter) can be inserted into the stomach. Withdraw the sheath and inflate the balloon. Snug the gastric wall up against the anterior abdominal wall by pulling back on the tube gently. It may be necessary to release some pneumoperitoneum to bring the anterior abdominal wall into closer apposition to the stomach.
T-fasteners (Fig. 58.1B) are a simple method to secure the stomach to the anterior abdominal wall. Place these by passing a needle through the anterior abdominal wall and stomach. Insert the closed T-fastener through the needle and snug it up. Alternatively, use a couple of simple sutures of 3-0 silk to tack the stomach to the anterior abdominal wall. Either method helps minimize the chance of leakage and increases the safety of the procedure by giving additional assurance that the stomach will be maintained in close apposition to the anterior abdominal wall during the healing phase.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


