Laparoscopic Appendectomy and Resection of Meckel Diverticulum
This chapter describes both laparoscopic appendectomy (including mobilization of the right colon for retrocecal appendix) and laparoscopic resection of Meckel diverticulum. Two methods of laparoscopic appendectomy—with and without the use of the endoscopic stapler—are presented.
SCORE™, the Surgical Council on Resident Education, classified laparoscopic appendectomy as an “ESSENTIAL COMMON” procedure.
STEPS IN PROCEDURE
Patient position, monitors placed to facilitate access to right lower quadrant
Three trocars most commonly used
Create pneumoperitoneum and explore abdomen
Grasp appendix and elevate
Expose base of appendix
Create window in avascular “sweet spot” at base of mesentery
Divide appendix with endoscopic stapler (gastrointestinal load)
Divide mesentery with endoscopic stapler (vascular load)
Remove small appendix through 10-mm trocar
Place large appendix in endoscopic bag for removal
Irrigate field, close any trocar sites greater than 5 mm
If Appendix Normal
Check pelvic organs (female)
Run small bowel for at least 121.92 cm (4 ft) to exclude Meckel diverticulum
Be guided by character and location of any fluid
HALLMARK ANATOMIC COMPLICATIONS
Injury to bowel or vessels during peritoneal entry
Injury to cecum during mobilization for retrocecal appendix
Missed pathology because of limited ability to palpate
LIST OF STRUCTURES
Cecum
Appendix
Mesoappendix
Appendicular artery
Terminal ileum
Meckel diverticulum
Setup and Initial View (Fig. 95.1)
Technical Points
Position the patient supine with both arms tucked in. Set the room up with the primary monitor at the patient’s right knee, and a secondary monitor, if desired, at the patient’s left knee. Palpate the abdomen. A palpable mass in the right lower quadrant generally implies complicated appendicitis; this can be managed laparoscopically if one is experienced.
Access the abdomen through a supraumbilical port. Inspect all four quadrants, looking for confirmation of the etiology. Aspirate and irrigate any purulent material, obtaining cultures if desired. If the appearance is consistent with appendicitis, place the operating table in Trendelenburg position with the right side elevated. The cecum should be visible in the right lower quadrant. Confirm cecum by taeniae and whiter color than adjacent loops of small intestine.
Place a working 5-mm port in the right upper quadrant at about the midclavicular line and pass an endoscopic Babcock clamp into the field. Gently retract the cecum toward the upper abdomen. The base of the appendix should roll into view. Note that the tip of the appendix is tethered by the mesoappendix, which passes
behind the terminal ileum. Additional ports will be placed in the left lower quadrant or lower midline (12 mm), depending on the size of the patient, and optionally in the right lower quadrant for additional retraction in difficult cases (Fig. 95.1A).
behind the terminal ileum. Additional ports will be placed in the left lower quadrant or lower midline (12 mm), depending on the size of the patient, and optionally in the right lower quadrant for additional retraction in difficult cases (Fig. 95.1A).
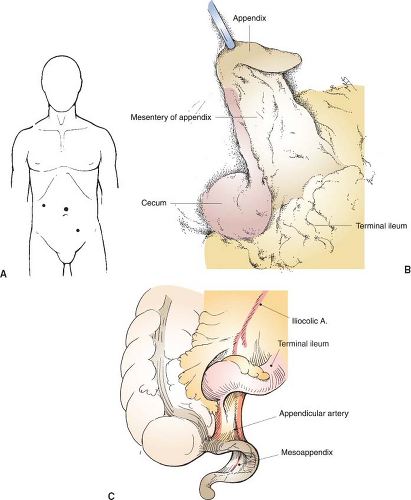 Figure 95.1 Setup and initial view. A: Trocar placement B: Initial view of appendix C: Regional anatomy (B from Scott-Conner CEH, Cuschieri A, Carter FJ, eds. Small intestine and appendix. In: Minimal Access Surgical Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2000:165–184, with permission; C from Wind GG. The colon. In: Applied Laparoscopic Anatomy: Abdomen and Pelvis. Baltimore, MD: Williams & Wilkins; 1997:217–246, with permission). |
Insert the 12-mm port next. If the patient is small, with a narrow abdomen, put this in the left lower quadrant, taking care to choose a site lateral to the rectus muscle to avoid the inferior epigastric vessels. If the patient is large, a lower midline site as shown will work well. As always, think in terms of working distance rather than fixed anatomic landmarks. Use an atraumatic grasper to manipulate cecum and appendix so that the appendix can be grasped by the Babcock clamp and elevated (Fig. 95.1B).
Anatomic Points
The outer muscular layer of the appendix is formed by longitudinal fibers, which are the continuation of the three taeniae of the colon. Thus the appendix may be located by seeking the convergence of the taeniae. Location of the appendix varies, but it is always tethered to some extent by the mesoappendix, which passes behind the terminal ileum (Fig. 95.1C). In many individuals, the appendix is partially or completely retrocecal.
The laparoscopic approach (base before tip) is different from that commonly used during open appendectomy. The laparoscopic surgeon has the advantage of working from within the abdomen and approaches the appendix from a vantage point cephalad and to the right. Thus as the cecum is pulled up, the base is the first part of the appendix to come into view. In all but the true retrocecal appendices (Fig. 95.4), the rest of the appendix generally then comes into view.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


