Laparoscopic Adrenalectomy— Lateral Approach
Geoffrey B. Thompson
Anna Kundel
DEFINITION
Lateral laparoscopic adrenalectomy is defined as a minimally invasive procedure to remove all or part of an adrenal gland via a lateral transperitoneal approach with the patient in a nearly full decubitus position.
ANATOMY
The adrenal glands lie partially anterior, medial, and superior to the upper pole of the kidneys. The caudal limb of the left adrenal gland often lies in close proximity to the left renal hilum.
The left adrenal vein frequently joins with the medially located inferior phrenic vein to form a common channel entering the left renal vein. This anatomic configuration, resulting in hormonal dilution within the common channel, is very important in understanding and interpreting the results of adrenal venous sampling (FIG 1).
The right adrenal vein is short, often wide, and empties directly into the posterolateral aspect of the inferior vena cava. On occasion, additional right adrenal veins may drain directly into the inferior vena cava or the right hepatic vein. Arterial inflow to the adrenals is less predictable but generally arises as small arteries originating from the renal artery (inferior adrenal artery), the aorta (middle adrenal artery), and the inferior phrenic artery (superior adrenal artery).
Paired small veins may accompany these arteries. It is these anatomic findings that allow for cortical-sparing adrenalectomy in familial pheochromocytoma syndromes, such as von Hippel-Lindau (vHL), neurofibromatosis type 1 (NF1), and multiple endocrine neoplasia type 2 (MEN-2) (FIG 2).
Rarely, small rests of adrenocortical tissue may be found at sites near the adrenal bed or within the gonads. This has particular importance when treating corticotropin-dependent hyperadrenocorticism.
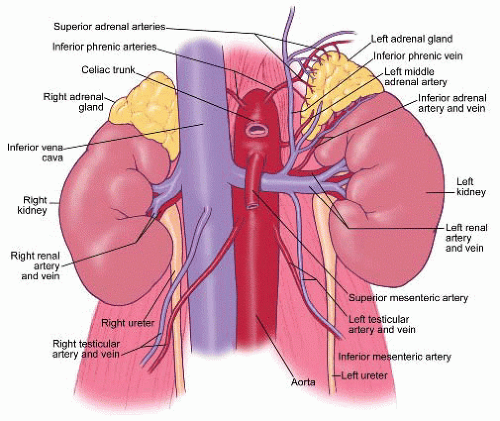 FIG 1 • Vascular anatomy of the adrenal glands. |
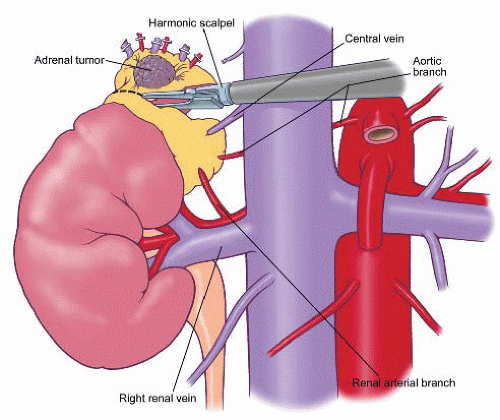 FIG 2 • Cortical-sparing adrenalectomy. |
PATHOGENESIS
Pheochromocytomas, aldosteronomas, and cortisol-secreting tumors produce catecholamines and hormones in an uncontrolled fashion, resulting in potentially life-threatening hormonal sequelae. Some of these tumors are seen in familial cases (MEN, vHL, NF1); most occur sporadically.
NATURAL HISTORY
Untreated functional tumors can lead to death and disability. Undiagnosed adrenocortical carcinomas are most often fatal.
PATIENT HISTORY AND PHYSICAL FINDINGS
Laparoscopic adrenalectomy is used for small functional and nonfunctional adrenal tumors, the latter being removed because of suspicion of underlying malignancy (either primary or metastatic).
Adrenal incidentalomas are incidentally discovered (asymptomatic) adrenal masses, typically picked up on crosssectional imaging studies performed for some other reason. For example, a patient comes to the emergency room with renal colic and a computed tomography (CT) with stone protocol is performed, revealing a ureteral calculus and an incidentally discovered 4-cm right adrenal mass.
Indications for removal an adrenal incidentaloma include (1) a functional lesion because of the risk associated with excess hormonal sequelae; (2) a growing lesion or a lesion greater than 4 cm in diameter because of the risk of adrenocortical malignancy; or (3) an abnormal radiographic phenotype, which can be an indicator of an underlying malignancy.
Table 1: Absolute Contraindications to the Laparoscopic Approach
Obvious, large adrenocortical carcinomas
Pheochromocytomas >8 cm or clearly malignant pheochromocytomas associated with direct invasion, nodal metastases, or distant metastases
Extensive upper abdominal surgery in which the surgeon should consider a posterior endoscopic approach (see Part 5, Chapter 49 )
Absolute contraindications to the lateral laparoscopic approach are described in Table 1.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Diagnostic Studies
Evaluation of an adrenal incidentaloma should include a 24-hour urine collection for fractionated catecholamines and total metanephrines or plasma metanephrines and normetanephrines.
In patients who are hypertensive, regardless of their serum potassium level, plasma aldosterone concentration (PAC) divided by plasma renin activity (PRA) should be calculated to screen for primary aldosteronism. In the case of a high PAC:PRA ratio, confirmation of primary aldosteronism is obtained by salt loading and demonstration of a failure to suppress urinary aldosterone in a 24-hour sample. Autonomous cortisol secretion should be ruled out with an overnight 1 mg or 8 mg dexamethasone suppression test. The demonstration of autonomous cortisol secretion is confirmed by a two-day low-dose dexamethasone suppression test.
Other studies available include a 24-hour urinary free cortisol level or demonstration of loss of diurnal variation between a.m. and p.m. plasma cortisol levels.
Midnight salivary cortisol levels are also being used with increasing frequency for case detection of cortisol hypersecretion.
Studies for estrogen and androgen excess are obtained when clinically indicated but are not routinely done.
Imaging
Imaging of pheochromocytomas (FIG 3), aldosteronomas, cortisol-secreting tumors, and adrenocortical carcinomas is best performed with CT or magnetic resonance imaging (MRI). Tumors that are round, homogeneous, and low in Hounsfield units on CT scan with rapid washout of intravenous contrast are thought to represent lipid-rich cortical adenomas (FIG 4).
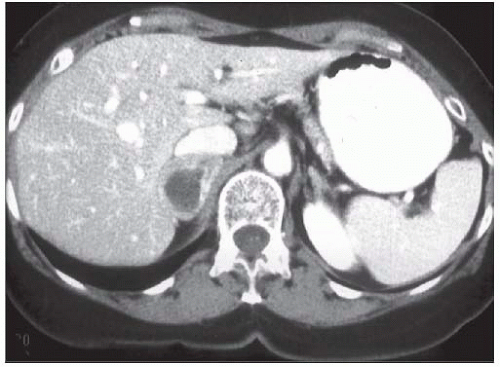
FIG 3 • CT scan of pheochromocytoma.
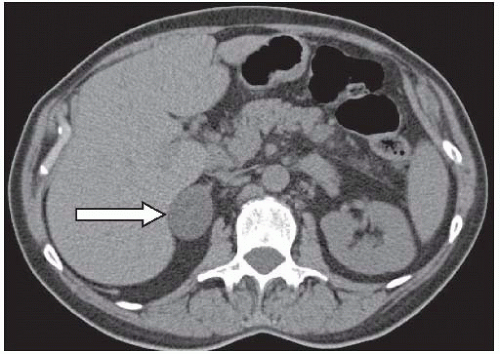
FIG 4 • CT scan of benign cortical adenoma.
Malignancies tend to be large and heterogeneous, with areas of hemorrhage or necrosis associated with high Hounsfield units on CT and delayed washout of intravenous contrast (FIG 5). These lesions appear bright on T2 weighted MRI images.
Approximately 25% of lesions 6 cm and greater are likely to be malignant, whereas 6% of lesions between 4 and 6 cm turn out to be primary malignancies. It is for this reason that the 4-cm cutoff is used. This avoids taking out an excessive amount of nonfunctional cortical adenomas while missing very few adrenocortical carcinomas.
CT imaging is also valuable in picking up small aldosteronomas, but because of the high incidence of nonfunctional incidentalomas in patients older than 50 years of age, adrenal venous sampling has become the localizing procedure of choice for determining lateralization of an aldosteroneproducing adenoma or hyperplasia.
Metaiodobenzylguanidine (MIBG) scanning is useful for detecting occult pheochromocytomas, paragangliomas, metastatic disease, and multiple tumors in familial cases.
 FIG 5 • CT scan of left adrenocortical carcinoma. |
NONOPERATIVE MANAGEMENT
Pheochromocytomas can be managed, albeit less effectively, with medical blockade (α-blockers). Aldosteronomas can be treated with mineralocorticoid receptor blockers, but this is not an ideal choice for younger patients.
SURGICAL MANAGEMENT
Preoperative Considerations
Laparoscopic adrenalectomy via a lateral approach is indicated in the following circumstances:
All benign, functional adrenal masses less than 6 cm in maximal diameter (aldosteronomas, cortisol-secreting tumors) and pheochromocytomas less than 8 cm in diameter
All nonfunctional adrenocortical tumors greater than 4 cm but less than 6 cm in diameter
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


