Keratoacanthoma
David Cassarino, MD, PhD
Key Facts
Terminology
Keratoacanthoma (KA)
Very well-differentiated SCC variant
Etiology/Pathogenesis
Similar to other forms of SCC, typically related to chronic solar (UV) damage
Clinical Issues
Often dome-shaped with central keratinous plug
May reach large size, up to 10 cm (giant KA)
Excellent prognosis; vast majority of cases spontaneously regress
Head and neck most common, followed by arms, legs
Microscopic Pathology
Scanning magnification shows a large, nodular, well-differentiated tumor
Typically appears symmetric with central keratin-filled crater present
Large squamous cells with abundant dense eosinophilic-staining cytoplasm and enlarged, hyperchromatic to vesicular-appearing nuclei with prominent nucleoli
Prominent inflammatory infiltrate, usually with abundant eosinophils and neutrophils
Regressing lesions often show epidermal atrophy and bland cytologic features
Top Differential Diagnoses
Conventional well-differentiated SCC
Squamous cell carcinoma in situ (SCCis) (Bowen disease)
Verrucous carcinoma
 Clinical photograph shows a tumor with raised borders and a central, crateriform keratin-filled defect, consistent with a keratoacanthoma. (Courtesy S. Yashar, MD.) |
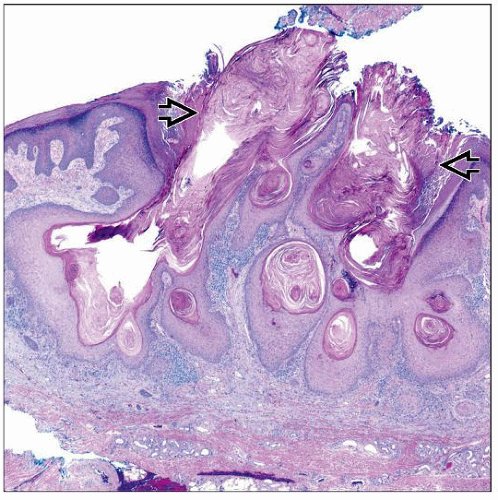 Scanning magnification of a keratoacanthoma shows an endophytic-appearing atypical squamous proliferation with prominent, central keratin-filled cavities  . . |
TERMINOLOGY
Abbreviations
Keratoacanthoma (KA)
Synonyms
Crateriform ulcer
Self-healing squamous cell carcinoma
Definitions
Very well-differentiated form of cutaneous squamous cell carcinoma (SCC), which often spontaneously regresses
ETIOLOGY/PATHOGENESIS
Environmental Exposure
Similar to other forms of SCC, typically related to chronic solar (UV) damage
Vast majority of lesions occur in sun-damaged skin of older adults
Regression is thought to be due to immune-mediated destruction of the squamous cells
CLINICAL ISSUES
Epidemiology
Incidence
Relatively common, may represent up to 25% of cases of cutaneous SCC
Age
Older adults, mean age is mid 60s
Gender
More common in males
Ethnicity
Most common in Caucasians
Site
Head and neck most common, followed by arms, legs
Presentation
Rapidly growing nodular lesion
Often dome-shaped with central keratinous plug
May reach large size, up to 10 cm (giant keratoacanthoma)
Treatment
Options, risks, complications
Surgical excision is mainstay of treatment although observation may be acceptable in many cases
Surgical approaches
Complete excision is curative but likely not necessary in most cases due to spontaneous regression
Patients with giant KAs, subungual KAs, and immunosuppressed patients should have complete excision, as lesions may not regress in these patients
Prognosis
Excellent; vast majority of cases spontaneously regress
Rare case reports of metastatic KA, but most of these are in giant or subungual KAs or immunosuppressed patients
MACROSCOPIC FEATURES
General Features
Typically large, scaly lesions with central keratinous crater
MICROSCOPIC PATHOLOGY
Histologic Features
Scanning magnification shows a large, nodular, well-differentiated squamous tumor
Lesion typically appears symmetric with central keratin-filled crater present
Cells may show infiltrative features at periphery of tumor
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


