Diarrhea is common, and it has been estimated that even in Western countries most experience at least two episodes of infectious diarrhea annually (see chapter on infections). It is generally considered chronic when the symptoms last more than 4 weeks. However, to put this in perspective, in Western societies irritable bowel syndrome (IBS) is by far the most common cause of chronic diarrhea and the most common exit diagnosis from most gastroenterology clinics. Consequently, most biopsies from the large bowel are from patients with IBS, in whom colonoscopy has been carried out to ensure there is not a more treatable cause of diarrhea such as microscopic colitis or unsuspected chronic idiopathic inflammatory bowel disease (IBD).
Diarrhea is defined in adults by abnormal stool weight (>200 g per day), consistency (loose or liquid), and/or frequency (>3 times per day). It is a common symptom in adults and the prevalence of diarrhea is approximately 1% to 5%, making it a major cause of disability.1 The list of etiology for diarrhea is fairly long; however, the major causes include IBS, infections, systemic disorders, drug toxicity, immunemediated disease, malabsorption, microscopic colitis, and IBD. While a vast majority of diarrhea is acute and self-limited necessitating no medical attention or investigations, patients with chronic diarrhea with or without the passage of blood are likely to be further investigated, often with some form of endoscopy and biopsy. Several studies show that colonoscopy with biopsy is useful in the investigation of patients with chronic diarrhea yielding a histological diagnosis in 22% to 31% of patients despite macroscopically normal colon at colonoscopy.2, 3, 4 A study evaluating more than 800 patients with chronic diarrhea who underwent colonoscopy with biopsy found that 122 (15%) of them had abnormal histopathology,3 which still means that 85% of patients had normal biopsies. Of those with abnormal biopsies, 2% would have been missed if only a flexible sigmoidoscopy had been performed. In patients older than age 50 years, colonoscopy is the method of choice.2, 3, 5, 6, 7, 8 However in a further study, 15% to 20% of patients with diarrhea-predominant IBS had features of microscopic colitis on biopsy.9 In most patients, colonoscopy shows mucosal abnormalities and the histological diagnoses include IBD, a variety of infections, systemic disorders, and drug-induced mucosal injury, among many others. However, various forms of colitis can be present in the absence of radiological and endoscopic evidence of colitis as shown in Table 18-1. Because the patterns of tissue response are limited despite a varied range of insults, the precise histological diagnosis of colitis requires a good knowledge of the different etiologies and of the microscopic features of different types of colitis.10, 11, 12, 13 This chapter discusses the major important causes of chronic diarrhea which include microscopic colitis and IBD. Readers are referred to other sections for the discussion of other major causes like infections (Chapter 19), immunodeficiency disorder (Chapter 3), malabsorption syndromes (Chapter 17), and drug toxicity and systemic disorders (Chapter 8).
Table 18-1 Normal Colonoscopy and Abnormal Histology
Infections
Spirochetosis
Miscellaneous infections: C. difficile, Campylobacter, E. coli, etc.
Drug-related or iatrogenic
Pseudomelanosis coli (mild)
Drug-related lymphocytic and collagenous colitis
Bowel prep artifacts
Miscellaneous
Inflammatory bowel disease (Crohn’s disease and ulcerative colitis)
Minimal change colitis
IBD in remission (quiescent colitis)
Microscopic colitis
Lymphocytic colitis
Collagenous colitis
Mastocytic (entero) colitis
Allergy-associated colitis
Eosinophilic cryptitis/colitis
MICROSCOPIC COLITIS
Introduction
The concept of “microscopic colitis” evolved from recognition that in some patients with chronic diarrhea, despite normal colonoscopy, inflammatory changes could be seen on microscopy. The term, microscopic colitis itself was used initially in 1980.14 It was subsequently shown that the most distinctive feature of this condition was a marked increase of the number of intraepithelial lymphocytes (IEL).15 The condition was therefore renamed “lymphocytic colitis.” It appeared to be different from “collagenous colitis,” a condition first reported in 1976. In this report, rectal biopsies from a woman with chronic watery diarrhea and an endoscopically normal rectal mucosa revealed a markedly thickened subepithelial collagen layer along with an increase in the lamina propria inflammatory cells.16 In 1993, a French and an American research group suggested the use of “microscopic colitis” as an umbrella term to cover any form of colitis in which there was histological, but no endoscopic or radiological abnormality.17, 18 Collagenous colitis and lymphocytic colitis were the two major types of microscopic colitis to be recognized. Since then, various other forms of colitis have been described,19, 20, 21, 22, 23, 24 some of which are variants of these two disorders, while others appear to be distinct nosological entities.25, 26, 27, 28, 29, 30 However, in current practice the use of the term “microscopic colitis” largely implies either collagenous or lymphocytic colitis and their variants, and the other conditions like eosinophilic colitis or possibly mastocytic enteropathy are designated by their specific names.
As is clear, the diagnosis of microscopic colitis requires clinicopathologic correlation (normal endoscopy, abnormal histology). A typical patient has a chronic intermittent disease course with watery diarrhea and characteristic microscopic features on biopsy. The clinicopathologic feature of collagenous colitis and lymphocytic colitis are very similar and hence discussed together, but they are not identical and some patients may even show overlapping features (discussed later). Whether these two are distinct entities or represent ends of a spectrum remains unresolved at present.
Epidemiology
The vast majority of reported patients with microscopic colitis have been from countries in Europe and North America and only a few series have been reported from Africa, Asia, Australia, and South America. It is estimated that about 10% of patients evaluated for chronic nonbloody watery diarrhea with colonoscopy appear to have microscopic colitis.31, 32 Incidence studies are rare. In a Swedish study, the mean annual incidence of collagenous colitis was 1.8 per 105 inhabitants. The median age at diagnosis was 64 years and the female to male ratio was 9:1.33 In a population-based study from Calgary, Canada from 2002 to 2004, the annual incidence was 10.0 per 105 person (lymphocytic colitis, 5.4; collagenous colitis, 4.6 per 100,000). Patients older than 65 years were five times more likely to develop microscopic colitis (RR, 5.6; 95% confidence interval [CI], 4.0-7.7). Women were at higher risk of acquiring microscopic colitis for both collagenous colitis (RR, 3.44; 95% CI, 2.07-5.97) and lymphocytic colitis (RR 6.29; 95% CI, 3.21-13.74). Elderly women with a history of malignancy were also associated with a higher risk of microscopic colitis (RR, 3.59; 95% CI, 1.68-7.01), as were patients with celiac disease (RR, 7.9; 95% CI, 4.0-14.2) and hypothyroidism (RR, 6.1; 95% CI, 3.5-10.0).34 In a population-based study from Olmsted County, Minnesota from 1985 to 2001, the annual incidence was 8.6 cases per 105 persons. There was a significant secular trend, with annual incidence increasing from 1.1 per 105 early in the study to 19.6 per 105 by the end (p < 0.001). Rates increased with age (p < 0.001). By subtype, the incidence was 3.1 per 105 for collagenous colitis and 5.5 per 105 for lymphocytic colitis. In this study, collagenous colitis was associated with female gender (p < 0.001), but lymphocytic colitis was not. Prevalence (per 105 persons) calculated on the last day of the study (December 31, 2001) was 103.0 (39.3 for collagenous colitis and 63.7 for lymphocytic colitis).35 Overall, it appears that the incidence of microscopic colitis is rising; among microscopic colitis, lymphocytic colitis appears to be more common than collagenous colitis and the predilection for female gender is stronger in collagenous colitis compared to lymphocytic colitis.
Etiology and Pathogenesis
The etiology of lymphocytic colitis and collagenous colitis is largely unknown and is probably multifactorial. It is suggested that they represent disorders with an abnormal mucosal immune response in predisposed individuals to various noxious luminal agents that include infections and toxins/medications. Many medications have been associated with lymphocytic (especially) and collagenous colitis, of which common ones include nonsteroidal anti-inflammatory drugs (NSAIDs), lansoprazole and ticlodipine (Table 18-2).36 In one study, 37.5% of patients taking long-term steroids and having diarrhea had lymphocytic colitis.37 While many of the drugs listed are known to cause or exacerbate diarrhea, these are also very commonly used drugs, and case-control studies clearly establishing an etiologic relationship are still lacking. In one review of 104 patients with microscopic colitis, about 35% of patients reported NSAID use.38 There are considerably fewer cases of drug-associated collagenous colitis compared to lymphocytic colitis.36
Table 18-2 Medications Potentially Related to the Development of Lymphocytic Colitis
Aspirin
Other NSAIDs
Ticlopidine
Lansoprazole
Bupropion
Sertraline
Colchicine
Etanercept
Carvedilol
Metformin
Omeprazole
Valproic acid
Amitriptyline
Troglitazone
Niacin
Hydroxychloroquine
Cisapride
Table 18-3 Autoimmune Disorders Associated with Microscopic Colitis
Many autoimmune or systemic inflammatory diseases are associated with microscopic colitis suggestive of a role for autoimmune or immune deregulation in the etiopathogenesis (Table 18-3).39, 40, 41, 42, 43 Collagenous colitis has also been reported to occur rarely as a paraneoplastic phenomenon in a patient with colon cancer, which resolved following tumor resection.44
Enteric infections such as Clostridium difficile, Campylobacter jejuni, and Yersinia enterocolitica have also been associated with the onset of microscopic colitis,45, 46, 47 and anecdotally, we have seen the same with collagenous colitis. A condition with histopathologic resemblance to lymphocytic colitis is “Brainerd diarrhea,” an outbreak of chronic watery diarrhea characterized by acute onset and prolonged duration, for which an infectious cause has been suggested (see later).13 Symptoms in lymphocytic colitis seems to occur more frequently in summer and fall, and this seasonal variation suggests a possible etiologic role of infections.48 Interestingly, a few cases of collagenous colitis with concomitant Helicobacter pylori gastritis have been reported that had resolution of diarrhea following treatment of H. pylori.49, 50 Immunologic response to H. pylori antigen has been postulated as a possible mechanism. Benefit from probiotic therapy in patients with collagenous colitis suggests that altered gut flora may also play a role in its pathogenesis in some patients.51 Genetically engineered mice that express HLA-B27 routinely develop lymphocytic colitis-like picture, but not in the absence of luminal bacteria.52 The postdysenteric IBS also mimics lymphocytic colitis. In this condition, the number of IEL can increase and decrease over time, in common with CD3+ lymphocytes in the lamina propria.10
Rare examples of familial cases have been described with both collagenous and lymphocytic colitis suggesting a role for genetic factors.53, 54 Increased frequency of HLA-A1 and a decreased frequency of HLA-A3 have been reported in lymphocytic colitis compared to controls and patients with collagenous colitis.55 Interestingly HLA-B27, which is commonly associated with other autoimmune disorders is not linked with microscopic colitis. NOD2/CARD15 gene polymorphisms that are associated with IBD are also not involved in the susceptibility to collagenous colitis.56
Celiac disease has also been associated with microscopic colitis, especially lymphocytic colitis. In a study by Wolber et al.,57 12 out of 39 (31%) patients with newly diagnosed celiac disease had a simultaneous diagnosis of lymphocytic colitis. Gluten-free diet in ten of these patients resulted in a clinical improvement in nine. Rectal gluten challenge in patients with celiac disease has shown a rapid increase of the number of IEL in the rectum.58 It is thus likely that gluten is somehow responsible for the histopathologic changes of lymphocytic colitis in some patients with celiac disease.
Other noxious luminal factors (chemical toxins or bacteria) may also be responsible for microscopic colitis, as in one study fecal diversion with ileostomy or sigmoidostomy led to a clinical and histologic remission in all patients (n = 9) of collagenous colitis, and closure of the ostomy resulted in disease recurrence in all.59 Bile salts could be one of the luminal factors, as bile-binding resins like cholestyramine have beneficial effects in a subset of patients.60, 61, 62 In one remarkable case of gall bladder to transverse colon fistula seen by us, collagenous colitis was seen in the colon distal to the fistula only. Resolution of diarrhea was seen immediately following closure of the fistula, suggesting a role for bile in the pathogenesis of collagenous colitis.
The mechanism of diarrhea appears to be multifactorial and could be osmotic, secretory, or both.63 Diarrhea may continue with fasting or elemental diet. Some patients have steatorrhea, likely related to smallbowel involvement. The pathophysiology has been studied mainly in collagenous colitis.64 Most attention has been focused on the subepithelial collagen layer, epithelial barrier function, and on the presence of lamina propria, eosinophils, and mast cells. Thickened subepithelial collagen layer has been suggested to result in a diffusion barrier. Thickening of the collagen layer can be caused by overproduction, reduced degradation, or a combination of both. Overproduction is supported by the immunohistochemical finding of an increased expression of the myofibroblast marker a-smooth muscle actin and the increased expression of procollagens shown by in situ hybridization. Reduced matrix degradation is supported by the reduced expression of the collagenase matrix-metalloproteinase (MMP)-1 and increased expression of tissue inhibitor of metalloproteinase-1 (TIMP-1).65 A rare case of collagenous colitis associated with osteogenesis imperfecta, which is an inherited disorder of collagen synthesis has also been reported.66 Decreased expression of occludins and claudin-4 has been shown in collagenous colitis suggesting defects of epithelial barrier function in collagenous colitis.64 Increased expression of TGF-β1 in eosinophils, cyclooxygenase-2 (COX-2) in macrophages, connective tissue growth factor (CTGF) in myofibroblasts, mucosal basic fibroblast growth factor (bFGF), increased mucosal expression of vascular endothelial growth factor (VEGF), and increased endoluminal nitric oxide have all been reported in collagenous colitis.67, 68, 69, 70, 71 A reduced expression of CD1d has been shown in colonic epithelium of patients with microscopic colitis.72 CD1d is a major histocompatibility complex class I—like molecule, which is involved in regulating normal immunity of the gastrointestinal tract (GI) and thus disordered mucosal immunity may play a role in the pathogenesis. Active collagenous colitis is also associated with a TH1 and interferonγ mucosal cytokine profile, similar to patterns found in celiac disease.73 Number of eosinophils and mast cells are increased in microscopic colitis. Eosinophil activation may affect mucosal permeability.74, 75 Also, increased production of histamine by mast cells may promote diarrhea.76
The thickened collagen layer may contribute to disturbed water and electrolyte absorption; however, there is no correlation of the thickness of the collagen layer with the severity of diarrhea, and diarrhea may persist despite disappearance of the subepithelial collagen layer.60, 77 On the other hand, thickened subepithelial collagen layer may be still be present despite disappearance of diarrhea or never having one.60 It is also possible that increase in subepithelial collagen layer is a mere morphological marker of the disease with very little role in the pathophysiology of the diarrhea. The situation is similar with lymphocytic colitis. In one study, follow-up biopsies in 13 patients with lymphocytic colitis, who had achieved remission and were symptom free, persistent lymphocytic colitis and mild nonspecific inflammation were present in 3 patients each, while 5 showed completely normal histology and 2 had interestingly converted to collagenous colitis.60 In the same study, follow-up biopsies of 10 patients with collagenous colitis, who were in remission and symptom free, showed persistent changes in 8, normal histology in 1, and change to lymphocytic colitis in 1 patient. This either suggests lag between clinical and histologic remission or a lack of correlation between histologic changes with symptoms.
Clinical Features and Endoscopic Findings
The typical presentation of microscopic colitis is chronic intermittent watery diarrhea. Weight loss and abdominal pain are less prominent. About one fourth of the patients may have nocturnal diarrhea. Rare cases may develop protein-losing enteropathy.78 Some patients do not have diarrhea.43 The clinical features of patients with lymphocytic colitis are less homogeneous. Overall, the age at onset, clinical symptoms, laboratory data, and occurrence of associated diseases are similar to patients with collagenous colitis, but with slightly older age of onset, less stronger females predilection, and shorter disease history.60 Blood in the stool is not a typical feature, so its presence should lead the clinician into considering other differentials. Routine blood tests are not diagnostic. Collagenous colitis patients have a higher prevalence of antinuclear, antigliadin, and anti-Saccharomyces cerevisiae antibodies than patients with lymphocytic colitis and controls (patients without GI disorders); however, these are diagnostically not useful.43, 79, 80
Radiographic and endoscopic examinations are normal or show nonspecific abnormalities. Mucosal granularity and irregularity of the rectosigmoid on double-contrast barium enema have occasionally been reported in collagenous colitis.81 Although classically there is no endoscopic abnormality, in practice, erythema or edema have been reported in up to one third of cases.
Microscopic Pathology
The major features and differences between collagenous colitis and lymphocytic colitis are summarized in Table 18-4.
Collagenous colitis. Collagenous colitis is characterized by the combination of a chronic colitis (plasma cells) and thickening of the subepithelial collagen layer (Figs. 18-1 and 18-2). Architecture is normal, although a minor degree of architectural distortion, as well as Paneth cell metaplasia, is common. However, these are rarely severe enough to confuse with IBD. Variable degree of mucosal inflammation is often present, being minimal in some cases, usually in the resolving phase. The thickness of the subepithelial collagen layer consisting of basement membrane in the normal colorectal mucosa is <4 µm with minor regional variations. It normally appears to be slightly thicker in the right side of the colon compared to the left and the normal values reported in the literature vary between 2-3 and 3-7 µm.82 Most studies suggest a minimum thickness of 10 µm of the subepithelial collagen layer for a diagnosis of collagenous colitis, although it usually measures 15 to 30 µm, or more (up to 70). One needs to be careful when interpreting a tangential section, where the basement membrane may artifactually appear thicker (Fig. 18-3A).
Table 18-4 Comparison of Collagenous and Lymphocytic Colitis
LYMPHOCYTIC COLITIS
COLLAGENOUS COLITIS
Clinical and Demographic Features
M:F
1:1 to 5:1
1:4 to 1:6
Associated autoimmune diseases
25.9%
53.3%
Associated celiac disease
14.8%
20%
Rectal sparing
8%
43%
Histologic Features
Subepithelial collagen layer
<10 µm
>10 µm
Surface epithelium
Stripping of epithelium
[check mark]
[check mark]
Epithelial flattening
[check mark]
[check mark]
Lamina propria inflammation
Moderate to severe
Mild to severe
Increased IEL
Present
Variable
Crypt architectural distortion
None to mild
None to mild
Paneth cell metaplasia
None to mild
None to mild
Ileal involvement
Variable
Variable
Another common artifact is lighter staining of the subnuclear part of the cytoplasm of the surface epithelium that mimics a thickened collagen layer; however, closer look at higher magnification makes the differentiation fairly easy (Fig. 18-3B). Comparison with the size of nuclei of small lymphocytes or plasma cells (5-7 µm) is a rough guide for estimating thickness of subepithelial collagen layer (if thicker than two of these nuclei in a well-oriented part of the biopsy, one is usually in the pathological range). Actual measurement of the subepithelial collagen layer is seldom required to make a diagnosis, and there is no evidence that quantitative analysis improves the diagnostic accuracy.83 A cut-off of 10 µm as a diagnostic criteria has been chosen arbitrarily and cases with lessthickened subepithelial collagen layer (4-9 µm) in the presence of other supporting histologic findings likely represent cases of microscopic colitis, although as the thickening becomes less conspicuous, the distinction from lymphocytic colitis becomes almost arbitrary (Fig. 18-3C).84 The thickening of the subepithelial collagen layer may be patchy, both within a biopsy specimen as well as between specimens from different regions of the colon, usually being thickest in the transverse colon. Thickening increases toward the right side of the colon and can be absent in the sigmoid colon and rectum. The rectum is spared in approximately 30% to 40% of cases.85, 86 Thus, rectal biopsies alone may miss this disease. While initial workup of patients (with flexible sigmoidoscopy) to rule out microscopic colitis with four biopsies every 10 cm from the left colon may be appropriate, negative results should be followed up with a full colonoscopy.87 Also, initial evaluation may miss the diagnosis in a good number of cases (one fourth to one third), which may either be related to sampling or lack of fully developed histology at the time; hence, there is a role for repeat colonoscopy.31, 88
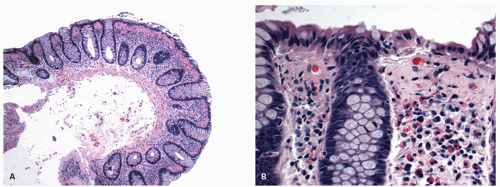
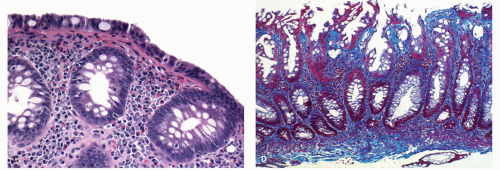
Figure 18-1. Collagenous colitis. A: Low-power view of an obvious example of collagenous colitis. Overview shows crypts with a normal architecture which may not extend as close to the muscularis mucosae as usual. The subepithelial collagen band, which occupies the upper quarter of the mucosa and measures about 60 µm in thickness, is apparent. B: High power: The luminal epithelium may be normal, but is often injured and cuboidal or low columnar with intraepithelial inflammatory cells. The inflammatory cells are mainly lymphocytes and are frequently very prominent. However, eosinophils and less frequently, neutrophils can be present. Also note the capillaries entrapped in the thick collagen layer; sometimes, when the thickness of the band is equivocal this feature may support a diagnosis of collagenous colitis.
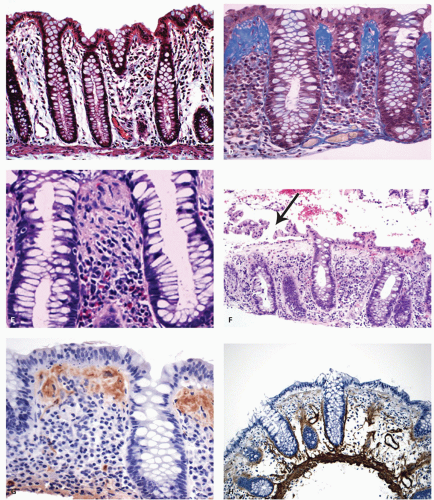
Figure 18-1.(Continued)C: Trichrome stain showing normal subepithelial and pericryptal collagen, as compared with markedly thickened subepithelial collagen in an example of collagenous colitis in (D). E: Sometimes, the eosinophils can be very prominent in the inflammatory infiltrate. F: Collagenous colitis with stripping of the surface epithelium (arrow). This is sufficiently characteristic of the disease that its presence should prompt immediate examination of the underlying collagen band, which here is greatly thickened. G: Immunostain for laminin shows strong positivity in the thickened subepithelial collagen, while staining for collagen type IV (basement membrane collagen) is negative (H).
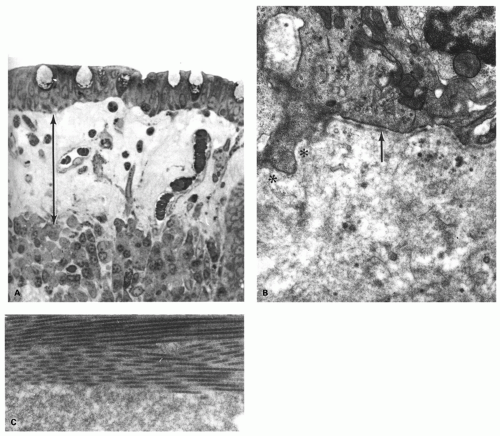
Figure 18-2. A: Electron micrograph of the subepithelial collagen layer. One mircometer epon section showing the thick subepithelial band and characteristic trapped capillaries underneath the epithelium. B: The basement membrane region (arrow) in collagenous colitis is commonly deficient focally (asterisk). The collagen layer itself consists of a mixture of amorphous ground substance and mature collagen. C: Detail to show the interface between the collagen fibers above and the ground substance below. (B and C, Courtesy of Dr. T.K. Shnitka.)
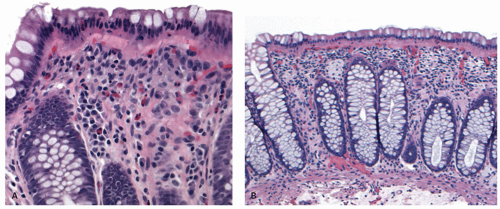
Figure 18-3. Possible errors in diagnosis. A: Tangential sectioning; the underlying crypts are visible in cross section, causing an artifactual impression of thickening of the collagen band. B: Nuclei of luminal epithelium are in the center of the cell, so that an eosinophilic zone is present beneath them, which can be mistaken for a thickened collagen band.
Figure 18-3.(Continued)C: Thickening of the subepithelial collagen that is <10 µm. Compare with the adjacent nuclei of lymphocytes. In the presence of increased IEL, lamina propria infiltrate, and epithelial injury, it certainly represents microscopic colitis, and a diagnosis of lymphocytic colitis would be favored. D: Marked thickening of subepithelial collagen in a hyperplastic polyp. Remaining colonic mucosa in this fragment and other colonic biopsies from this patient do not show any evidence of collagenous colitis.
Identification of the thickened subepithelial collagen layer is easy on H&E sections in most cases and can be highlighted with histochemical stains for collagen like the trichrome stain. Another simple method is to examine the H&E sections under a fluorescent microscope as the collagen is autofluorescent and the thickening of subepithelial collagen layer is immediately obvious.89 The SCL is composed of collagen type I, III, and VI in addition to the glycoprotein tenascin and is separated from the epithelial cells by the apparently normal basement membrane composed of collagen type IV (Fig. 18-1H
Only gold members can continue reading. Log In or Register to continue