Hodgkin Lymphoma of the Mediastinum
Key Facts
Clinical Issues
Asymptomatic in about 50% of patients (incidental finding on chest x-ray or CT scan)
More frequent in young patients; female predilection
Chest pain and dyspnea
Fever and night sweats (type B symptoms) present in about 30% of patients
Macroscopic Features
HL may involve mediastinal lymph nodes or thymus proper
When involving thymus, tumor tends to be well circumscribed and encapsulated
When involving thymus, cystic changes may be prominent in tumor
Microscopic Pathology
Nodular sclerosing subtype is most common variant encountered in mediastinum
Ill-defined, cellular nodules separated by broad bands of fibrous tissue
Admixture of small lymphocytes, plasma cells, eosinophils, histiocytes, and Reed-Sternberg cells and their variants
“Syncytial” variant of HL shows sheets of “lacunar” Reed-Sternberg cells surrounding areas of necrosis
Classical Reed-Sternberg cells are large, binucleated, and display characteristic “owl-eyed” large eosinophilic nucleoli
Mononuclear variants (Hodgkin cells) have large single nucleus with prominent eosinophilic nucleolus
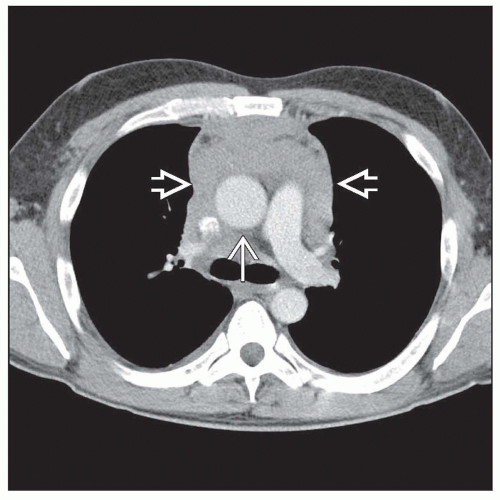 Axial contrast-enhanced CT shows a soft tissue anterior mediastinal mass  , which surrounds the aorta , which surrounds the aorta  and other vascular structures without obstruction. This is typical of Hodgkin lymphoma. and other vascular structures without obstruction. This is typical of Hodgkin lymphoma. |
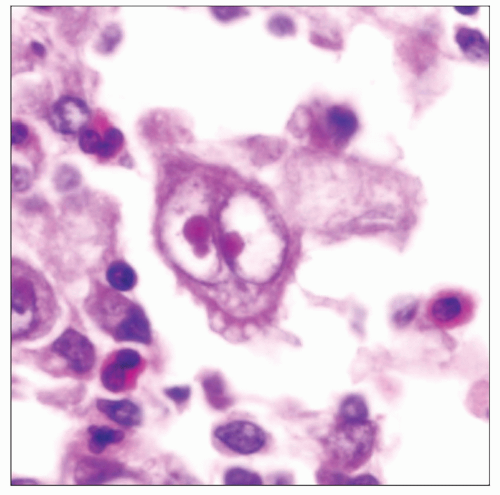 Classical Reed-Sternberg cell is seen in Hodgkin lymphoma (center of the field). Notice the large nuclei with prominent “owl-eyed” nucleoli and scattered eosinophils surrounding them. |
TERMINOLOGY
Abbreviations
Hodgkin lymphoma (HL)
Synonyms
Hodgkin disease
Classical Hodgkin lymphoma (CHL)
Definitions
Malignant proliferation of CD30/CD15(+) lymphoreticular cells of B-cell lineage intimately admixed with other reactive cellular elements arising within mediastinal lymph nodes &/or thymus
CLINICAL ISSUES
Presentation
Asymptomatic in about 50% of patients (incidental finding on chest x-ray or CT scan)
More frequent in young patients; female predilection
Chest pain and dyspnea
Advanced cases may present with superior vena cava syndrome
Fever and night sweats (type B symptoms) present in about 30% of patients
Disease may involve mediastinal lymph nodes, thymus, or both
Treatment
Radiation therapy is effective for patients in stages I and II
Advanced stages and bulky mediastinal disease require combination chemotherapy
Prognosis
Mediastinal HL is a curable disease for patients with stages I or II disease
Approximately 95% of patients with stage IA or IIA disease and small tumor burden will be alive and free of disease at 10 years
Patients who fail chemotherapy for advanced disease and suffer relapse have poor prognosis
IMAGE FINDINGS
General Features
Chest x-rays show solid, lobulated anterior mediastinal mass
Tumors can show multicystic changes on imaging studies
Prevascular and paratracheal lymph nodes are most commonly affected
CT Findings
Multiple rounded soft tissue masses or bulky soft tissue masses
Displacement, compression, and invasion of mediastinal or chest wall structures
MACROSCOPIC FEATURES
General Features
HL may involve mediastinal lymph nodes or thymus proper
When involving thymus, tumor tends to be well circumscribed and encapsulated
Nodular, gray-white, homogeneous and rubbery tissue on cut section
When involving thymus, tumor may show prominent cystic changes
Sections to Be Submitted
1 block per cm of largest tumor diameter
In cystic lesions, sample amply solid areas in cyst walls
MICROSCOPIC PATHOLOGY
Histologic Features
Nodular sclerosing subtype is most common variant encountered in mediastinum
Ill-defined, cellular nodules separated by broad bands of fibrous tissue
Admixture of small lymphocytes, plasma cells, eosinophils, histiocytes, and Reed-Sternberg cells and their variants
Epithelial-lined cysts containing solid areas with characteristic lymphoreticular proliferation in cyst walls
Entrapped, hyperplastic thymic epithelium can be encountered within tumor in cases arising in thymus
Sclerosis can be massive, resulting in large expanses of acellular collagenous stroma with small islands containing characteristic tumor cells
Pattern of sclerosis may be fine and reticular, resulting in “compartmentalization” of tumor cells reminiscent of diffuse large B-cell lymphoma of mediastinum with sclerosis
Syncytial variant of nodular sclerosis Hodgkin lymphoma
Sheets of “lacunar” Reed-Sternberg cells surrounding areas of necrosis
Cytologic Features
Identification of Reed-Sternberg cells is required for diagnosis
Classical Reed-Sternberg cells are large, binucleated, and display characteristic “owl-eyed” large eosinophilic nucleoli
Mononuclear variants (Hodgkin cells) have large single nucleus with prominent eosinophilic nucleolus
“Lacunar” Reed-Sternberg cells are characterized by clear halo surrounding nucleus
Reed-Sternberg cells may show bizarre forms due to extensive degenerative changes
Anaplastic tumor cells with abundant cytoplasm reminiscent of pleomorphic high-grade sarcoma
Degenerating cells with pyknotic, hyperchromatic nuclei (“mummy” cells)
ANCILLARY TESTS
Immunohistochemistry
Reed-Sternberg cells and their variants are positive for CD30 and CD15
Reed-Sternberg cells are negative for CD3, CD20, and CD45
DIFFERENTIAL DIAGNOSIS
Germ Cell Tumor
Seminoma, embryonal carcinoma, yolk sac tumor
Elevated oncofetal proteins (AFP, PLAP, HCG, etc.) in serum
Absence of regional or generalized lymphadenopathy
Absence of Reed-Sternberg cells
Thymoma
Epithelial cells in thymoma are devoid of cytologic atypia or multinucleation
Monotonous lymphoid cell infiltrate (immature T cells) seen in thymoma
Absence of Reed-Sternberg cells in thymoma
Large epithelioid cells in thymoma stain for cytokeratin rather than for CD30
Diffuse Large Cell Lymphoma (DLCL) of Mediastinum
Pattern of sclerosis in DLCL is characterized by small compartments rather than large lobules
Neoplastic cell population is more uniform than in HL, without eosinophils, histiocytes, and plasma cells
Atypical tumor cells in DLCL are positive for CD20 and CD45 and negative for CD15 and CD30
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


