History of Therapeutic Approaches to Acid Related Diseases
The evolution of therapy
|
Prout initially identified gastric acid as hydrochloric acid in 1823. However, it was only in the late nineteenth century that hyperchlorhydria was recognized as contributing to ulcer generation. For centuries, treatment had not changed. Only as pathogenesis and stimulatory pathways became recognized did surgical and then medical therapy become more focused and more effective.
Diet
In 1915, Dr. Bertram Sippy advocated hourly feedings of milk, eggs, and purees from 7:00 a.m. to 8:00 p.m. Between these hourly feedings, and every half hour for 2½ hours after the last feeding, Sippy powder (calcium and sodium bicarbonate) was administered. In addition, to relieve dyspepsia, the patient’s stomach was aspirated at regular intervals each night. This regimen provided a challenge both for the patient and for the nursing staff.
An alternative dietary therapy developed by Richard Doll involved the use for up to 3 weeks of continuous milk drips through a nasogastric tube, with or
without alkali. Although this therapeutic strategy seemed to improve the nutritional status of his patients, the obsessive need for dietary management and regulation of alkali intake so interfered with the lifestyle of patients and so often failed to prevent complications from developing that even surgery became a reasonable option.
without alkali. Although this therapeutic strategy seemed to improve the nutritional status of his patients, the obsessive need for dietary management and regulation of alkali intake so interfered with the lifestyle of patients and so often failed to prevent complications from developing that even surgery became a reasonable option.
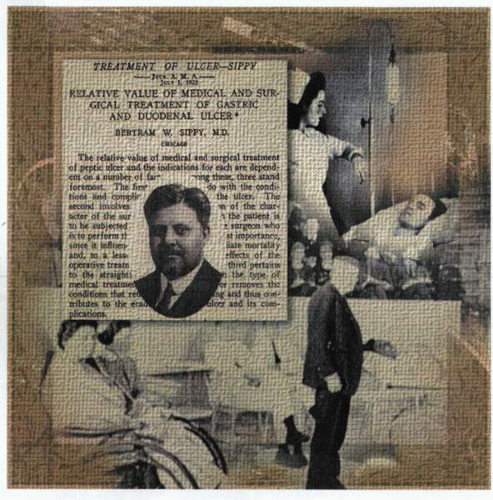 Dr. Bertram Sippy of Chicago (left) devised a complex dietary regimen of bland food that included hourly feedings of milk, eggs, and puree as well as the administration of large quantities of calcium and sodium bicarbonate. In addition, he proposed that particularly severe nocturnal dyspepsia could be relieved by regular gastric aspiration. Although cumbersome and likely to generate obsessive-compulsive disorders, this strict regimen was of some benefit and particularly efficacious when compared with the outcome of current surgical intervention for acid peptic disease. Many physicians (bottom) enthusiastically attended lectures by Sippy to learn more of his novel therapeutic techniques. An alternative dietary therapy developed by Richard Doll proposed hospital admission for up to 3 weeks with continuous nasogastric milk infusion with and without alkali (top right). Although this therapy promoted ulcer healing and relieved pain, the prolonged hospitalization and use of resources, as well as loss of productive work time, generated a less than optimal solution for the management of acid peptic disease. Cynics proposed that the excessive use of milk accelerated coronary artery disease, and that any putative therapeutic benefit was actually derived from the bed rest, the charm of the nursing staff, and the Freudian benefits of the acquisition of milk. This treatment soon fell into disregard except among unusual sects of medical practice. |
Surgery
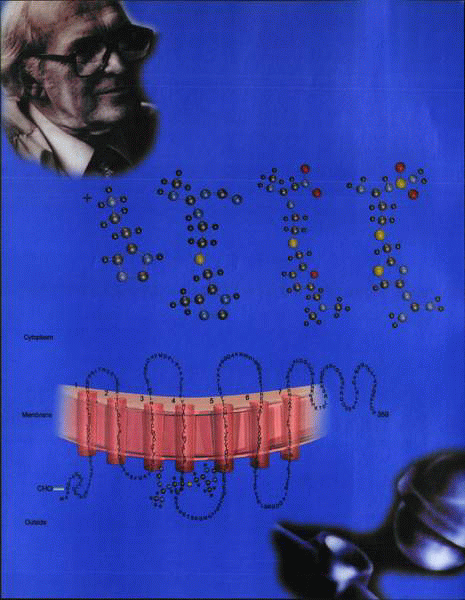
The first dedicated operation was a gastrectomy, but the high morbidity and mortality engendered a degree of caution in both patient and physician alike. Subsequently, vagotomy, which had been initiated in France by Raymond Latarjet and then reactivated in North America by Lester Dragstedt, provided a better alternative for management. Dragstedt’s observations that gastric acid output was decreased by vagotomy were widely cited in favor of this operation. Initial postoperative problems due to decreased gastric emptying were subsequently obviated by the construction of a variety of pyloroplasties to facilitate drainage. Recurrence of peptic ulcer disease and the long-term side effects of the surgery itself show that this therapy option was suboptimal.
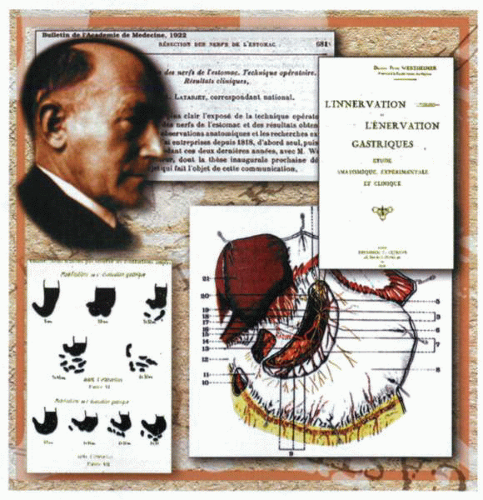 Andre Latarjet (1877-1947) (top left) was born in Dijon and studied medicine in Lyons. In collaboration with Pierre Wertheimer, he defined the neural innervation of the stomach in detail and recognized that the vagal nerve supply to the lesser curve was critical in the regulation of gastric acid secretion (top). In 1923, he published the results of a series of operations (right) in which he had severed the vagal nerves to the stomach and demonstrated not only a decrease in gastric acid secretion but also a resolution of acid peptic disease (bottom). A rigorous scientific thinker, he documented the associated significant delay in gastric emptying consequent on vagal denervation and described the need to add a drainage procedure to the operation. Lester Dragstedt introduced the vogue for vagotomy in the United States on January 14, 1943, in Chicago, at the Merritt Billings Hospital. As a transmogrified physiologist, Dragstedt was able to provide experimental evidence that gastric denervation decreased acid secretion and facilitated ulcer healing and relief of pain. It has taken almost 50 years for the surgical community to recognize that Latarjet’s original decision to abandon the operation was well founded on scientific fact. The long-lasting dramatic postvagotomy symptomatology consequent on denervating large portions of the gastrointestinal tract far outweighed the modest advantages achieved by a 20% to 30% decrease in acid secretion. Further debate on the merits and demerits of the innumerable permutations and commutations of vagotomy were swept away by the introduction of H2 receptor antagonists in 1976. The subsequent availability of PPI therapy considerably decreased the use of vagal resection, which should now only be considered in rare clinical circumstances. |
Gastroprotection
The evolving trend to use less invasive methodology in the management of peptic ulcer disease resulted in a significant interest in the use of antacids in association with both diet modification and bed rest.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


