Hidradenocarcinoma
Christine J. Ko, MD
David Cassarino, MD, PhD
Key Facts
Terminology
Malignant acrospiroma, malignant hidradenoma
Malignant adnexal tumor arising from, or showing areas similar to, a hidradenoma
Clinical Issues
Most frequently occurs on head and neck region
Presents as nodule or mass lesion
Excision is sometimes curative
Mohs micrographic surgery may be best option to ensure clear margins
Course can be aggressive, with local recurrences and metastases
Microscopic Pathology
Epithelial islands with interspersed glands/ducts
Cells composing islands are variable
Clear, poroid, squamoid (less common), rarely mucinous
Hyalinized stroma (similar to hidradenoma)
Infiltrative growth pattern (not well-circumscribed, unlike hidradenoma)
Deep extension
Perineural or vascular invasion may be present
Ki-67 generally shows a high proliferative index
Top Differential Diagnoses
Hidradenoma
Metastatic renal cell carcinoma
Clear cell squamous cell carcinoma
Clear cell basal cell carcinoma
Sebaceous carcinoma
Porocarcinoma
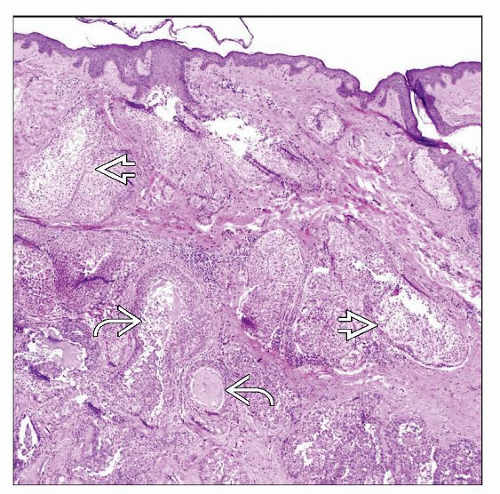 Low magnification of a hidradenocarcinoma shows a dermal-based, atypical, multilobular neoplasm with clear cell features  and cystic spaces and cystic spaces  containing mucinous material and cellular debris. containing mucinous material and cellular debris. |
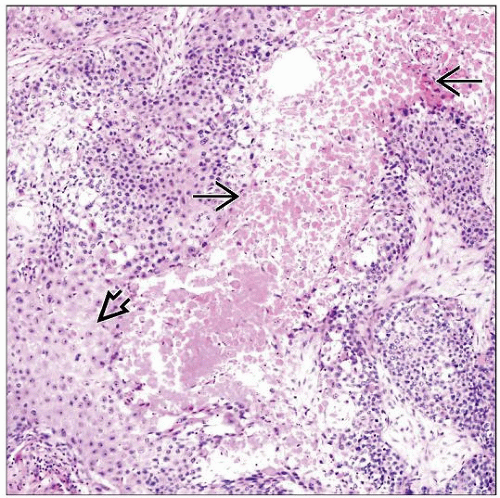 Areas of squamous differentiation  and prominent tumoral cell necrosis and prominent tumoral cell necrosis  are present in this example of hidradenocarcinoma. Squamous differentiation is much less common than in porocarcinoma. are present in this example of hidradenocarcinoma. Squamous differentiation is much less common than in porocarcinoma. |
TERMINOLOGY
Synonyms
Malignant acrospiroma, malignant hidradenoma
Definitions
Malignant adnexal tumor arising from, or showing areas similar to, a hidradenoma
CLINICAL ISSUES
Site
Most frequently in head and neck region
Presentation
Nodule or mass
Treatment
Surgical approaches
Wide, local excision of tumor
Mohs micrographic surgery may be best option to ensure clear margins
Drugs
For metastatic hidradenocarcinoma, if surgery is not an option
Various chemotherapeutic regimens reported
Case reports of sunitinib and capecitabine treatment
Radiation
Variable response
Prognosis
Excision is sometimes curative
Course can be aggressive
Local recurrences
Metastatic disease
Lymph nodes, distant skin, internal organs
MICROSCOPIC PATHOLOGY
Histologic Features
Epithelial islands with interspersed glands/ducts
Architecture may be predominantly solid islands; sometimes cystic areas present
Cells composing the islands are variable
Clear, poroid, less commonly squamoid, rarely mucinous
Hyalinized stroma
Infiltrative growth pattern; not well-circumscribed
Deep extension
Necrosis may be evident
Nuclear pleomorphism may be present
Mitoses often present
May be > 4 per 10 high-power fields
Perineural or vascular invasion may be identified
Area of tumor compatible with benign hidradenoma may be seen
Cytologic Features
May show high-grade cytologic atypia
Some cases may be composed of relatively bland cells without prominent cytologic atypia
Mitoses may be few or many
Varying proportions of clear, poroid, and squamoid cells
Poroid cells have dark blue nuclear outline with finely granular nucleoplasm
ANCILLARY TESTS
DIFFERENTIAL DIAGNOSIS



