Hepatocellular Carcinoma and Variants
Joseph Misdraji, MD
Laura Webb Lamps, MD
Key Facts
Etiology/Pathogenesis
Chronic viral hepatitis is leading cause of HCC worldwide
70-90% of HCC arises in cirrhosis
Clinical Issues
In USA, annual incidence is approximately 4 per 100,000
Most often presents with abdominal pain, malaise, weight loss, hepatomegaly
AFP is elevated in 70-90% of patients
In USA, 5-year survival is 30-40% overall, but 75% for tumors < 5 cm
Macroscopic Features
Typically soft, bile-stained with hemorrhage and necrosis
Can be solitary tumor, multiple discrete tumors, or small indistinct nodules throughout portion of liver
Gross venous or bile duct invasion occurs commonly
Microscopic Pathology
Grows as thickened hepatic plates separated by sinusoids without desmoplastic stroma
Tumor cells resemble hepatocytes with polygonal shape, round vesicular nuclei, and prominent nucleoli
Bile pigment in dilated canaliculi is helpful in distinguishing HCC from its mimics
Ancillary Tests
Positive for Hep-Par1, Glypican-3, and CAM5.2 (keratins 8 and 18)
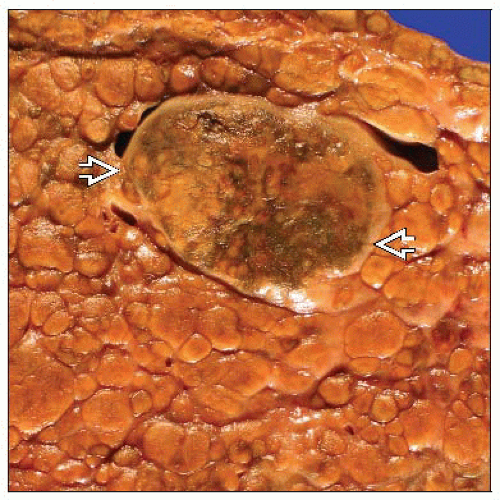 Gross photograph shows a large bile-stained tumor nodule  in a background of cirrhosis. This is a classic presentation of hepatocellular carcinoma. in a background of cirrhosis. This is a classic presentation of hepatocellular carcinoma. |
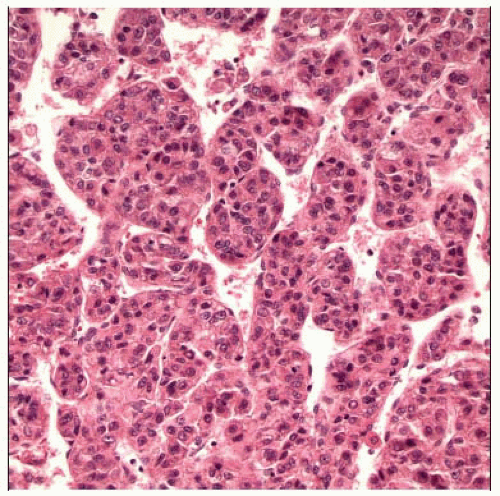 Hepatocellular carcinoma is typically composed of neoplastic cells resembling hepatocytes with a high nuclear to cytoplasmic ratio, which are organized into thick, disordered trabeculae. |
TERMINOLOGY
Abbreviations
Hepatocellular carcinoma (HCC)
Synonyms
Hepatoma
Definitions
Primary malignant neoplasm of liver with hepatocytic differentiation
ETIOLOGY/PATHOGENESIS
Developmental Anomaly
HCC can occur in patients with various congenital anomalies, including Alagille syndrome, ataxiatelangiectasia, Abernethy malformation, and bile salt export protein (BSEP) deficiency
Environmental Exposure
Aflatoxin B1, a mycotoxin produced by fungi of Aspergillus genus that contaminates food, is major cause of HCC in China and southern Africa
Alcoholic cirrhosis is major cause of HCC in western populations
Other exposures linked to HCC include anabolic steroids, Thorotrast, oral contraceptives, and smoking
Infectious Agents
Chronic viral hepatitis (hepatitis B and hepatitis C) is leading cause of HCC worldwide
Metabolic Disorders
Various metabolic disorders, including hemochromatosis, tyrosinemia, hypercitrullinemia, α-1-antitrypsin deficiency, and fructosemia, are associated with increased risk of HCC
Cirrhosis
70-90% of HCC arises in cirrhosis
Macronodular cirrhosis is more strongly associated with HCC than micronodular
Progression of Benign Tumor
HCC can arise in preexisting hepatocellular adenoma
CLINICAL ISSUES
Epidemiology
Incidence
Varies widely depending on geography in parallel with prevalence of hepatitis B and C and aflatoxin exposure
East Asia and southern Africa have highest incidence worldwide, up to 150 per 100,000
In USA, annual incidence is approximately 4 per 100,000
Age
Incidence increases with advancing age and then falls off in elderly; however, average age varies depending on geography
In parts of world with high incidence, average age is 35 years
In USA, average age is 60 years
Can occur in children, particularly in those with metabolic or genetic disorders
Gender
More common in men
Presentation
Abdominal pain due to stretching of Glisson capsule
Malaise, weight loss, hepatomegaly
Decompensation of previously stable cirrhotic patient with jaundice and rapidly accumulating ascites
Fever, leukocytosis, and liver mass mimicking hepatic abscess
Increasingly, small asymptomatic tumors are being found during surveillance of cirrhotic patients
Laboratory Tests
α-fetoprotein (AFP) is elevated in 70-90% of patients
Natural History
Metastasis occurs in 40-60% of patients
Most common locations are lymph nodes in porta hepatis, around pancreas, and celiac axis
HCC has tendency for intravascular spread with involvement of hepatic and portal veins
Hematogenous spread most commonly occurs to lungs, but also adrenal glands, bone, stomach, heart, pancreas, kidney, spleen, and ovary
Tumor seldom breaches Glisson capsule, and therefore dissemination throughout peritoneal cavity is rare
Treatment
Surgical approaches
Resection is possible if sufficient reserve liver function
Transplantation is option if patient meets “Milan criteria” of single tumor < 5 cm, or fewer than 4 tumors, none > 3 cm
Drugs
Sorafenib
Tyrosine kinase inhibitor that has proven to be at least somewhat effective in advanced cases
Ablation therapy
Radiofrequency or microwave ablation or direct percutaneous ethanol injections are options for small tumors
Angiographic embolization of hepatic artery can infarct tumor and prolong survival
Prognosis
Better prognosis associated with age < 50 years, female gender, resectable tumor, better differentiated tumor, low mitotic index, absence of vascular invasion, encapsulated tumor, and absence of cirrhosis
In USA, 5-year survival is 75% for tumors < 5 cm and 30-40% overall
MACROSCOPIC FEATURES
General Features
Soft tumor that can be bile-stained, with variable hemorrhage and necrosis
Can be solitary tumor, solitary tumor with “satellite nodules,” multiple discrete tumors, or multiple small indistinct nodules throughout portion of liver or entire liver
Pedunculated tumors are rare, more easily resected, and have better prognosis
Encapsulated tumors are rare, usually solitary tumors that arise in cirrhotic livers, and have better prognosis
Gross venous or bile duct invasion may be seen and should be sought
MICROSCOPIC PATHOLOGY
Histologic Features
Architectural patterns
Trabecular pattern: Tumor cells grow as thickened hepatic plates separated by sinusoids without desmoplastic stroma
Pseudoglandular or acinar pattern: Tumor cells grow in solid nests with central degenerative changes
Compact pattern: Trabeculae grow compressed together
Scirrhous pattern: Resemble trabecular HCC but with abundant stroma
Giant cell pattern: Multinucleate giant cells
Spindle cell pattern is often referred to as sarcomatoid HCC
Tumor cell morphology
Tumor cells resemble hepatocytes with polygonal shape, round vesicular nuclei, and prominent nucleoli
Inclusions can be seen in tumor cells, including Mallory hyaline, hyaline globules, and pale bodies
Clear cells may be present and even numerous due to accumulation of glycogen, water, or fat
Presence of bile pigment in dilated canaliculi is helpful in distinguishing HCC from its mimics



