Hand-assisted Laparoscopic Donor Nephrectomy
Stephen C. Rayhill
Preoperative studies have confirmed that the donor is anatomically suitable for kidney donation. The donor is typed and cross-matched for two units of packed red blood cells, and preoperative antibiotics are given. The patient is liberally hydrated throughout the procedure (about 4 L).
The left kidney is commonly selected because of the greater length of renal vein. A brief section at the end of this chapter describes the modifications necessary for the right kidney. This chapter describes a vertical midline incision for this purpose; others have described the use of a Pfannenstiel incision for kidney retrieval after a completely laparoscopic operation is completed. These alternative techniques are described in the references at the end.
Steps in Procedure
Right lateral decubitus position (for left donor nephrectomy)
Camera port 2 to 3 cm inferior and 5 cm to the left of the inferior margin of the umbilicus
Three additional trocars placed as shown in Fig. 91.1
Create hand-port incision in lower midline
Insert hand-port
Retract colon and spleen medially
Open Gerota’s fascia over anterolateral aspect of kidney
Establish plane between Gerota’s fascia and capsule
Open Gerota’s fascia superiorly
Identify ureter as it crosses iliac vessels
Dissect ureter and periureteral tissues
Complete dissection of Gerota’s fascia inferiorly, laterally, and medially
Retract colon mesentery to right of aorta to expose left renal vein
Clip and divide the left gonadal and adrenal veins
Divide lumbar vein with ultrasonic shears or clips (if large)
Expose and isolate the left renal artery to its juncture with the aorta
Dissect distal ureter, maintaining periureteral tissue
Doubly clip and divide distal ureter
Divide renal artery and vein with linear stapler (vascular cartridge)
Remove kidney through hand-port incision
Close incision and trocar sites in usual fashion
Hallmark Anatomic Complications
Ureteral devascularization
List of Structures
Left Kidney
Gerota’s fascia
Ureter
Aorta
Left renal artery
Inferior Vena Cava
Left renal vein
Left adrenal vein
Left gonadal vein
Lumbar veins
Right kidney
Iliac vessels
Gonadal vessels
Inferior epigastric artery
Rectus sheath
Colon
White line of Toldt
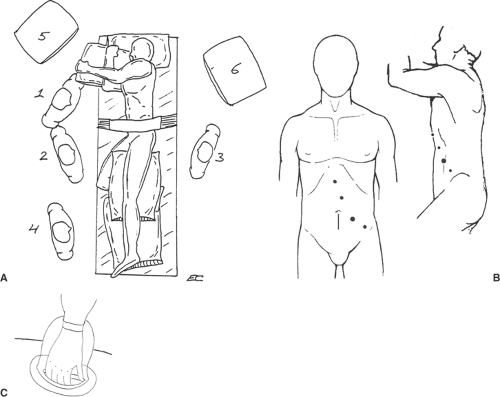 Figure 91-1 Incision and Placement of Trocars (A,B from Cho ES, Flowers JL. Laparoscopic live-donor nephrectomy. In: Zucker KA, ed. Surgical Laparoscopy. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2001:657–667, with permission; C from Soper NJ, Halpin VJ, Meyers BF. Minimally invasive surgery: laparoscopic and thoracoscopic techniques. In: Baker RJ, Fischer JE, eds. Mastery of Surgery. 4th ed. Philadelphia: Lippincott Williams & Wilkins, 2001:264–276, with permission.) |
Incision and Placement of Trocars (Fig. 91.1)
Technical Points
Place the donor in the right lateral decubitus position (right side down) and flex the table (Fig. 91.1A). Accurately plan and mark the following trocar sites and incision lines (Fig. 91.1B). The inferior medial (camera) trocar site is placed 2 to 3 cm inferior and 5 cm to the left of the inferior margin of the umbilicus (estimate the lateral edge of the hand-assist device to be sure to be lateral to it). The lateral trocar is placed 3 cm medial and 2 cm inferior to the iliac crest.
Make a 1.5-cm incision at the medial site (being careful not to burn the skin edges) and insert a Veress needle (or Hasson port). If adhesions are suspected, make the midline hand incision first (or use a Hasson port) and then place the ports under direct vision. Insufflate the abdomen and place the 12-mm medial trocar. Insert the laparoscope and place the 12-mm lateral port under laparoscopic guidance.
Next, create the midline hand-port incision. Draw a line beginning at the inferior edge of the umbilicus and extending 7 cm superiorly (depending on glove size) and make an incision just large enough to permit the hand. Insert the hand-port and subsequently use the left hand to retract the kidney atraumatically and facilitate dissection.
Anatomic Points
The inferior epigastric artery runs in the lateral aspect of the rectus sheath and should be avoided when placing the trocars.
Exposure of the Kidney (Fig. 91.2)
Technical Points
Incise the white line of Toldt laterally to the descending and sigmoid colon, beginning with the splenic attachments (Fig. 91.2A). Retract the colon medially (Mattox maneuver). Take care not to penetrate the colonic mesentery, which is often quite thin. Mobilize the spleen medially by dividing the splenorenal ligament (Fig. 91.2B). To provide maximal medial retraction of the descending colon, carefully divide the splenocolic attachments with ultrasonic dissecting shears. Open Gerota’s fascia over the anterolateral aspect of the kidney and establish the plane between Gerota’s fascia and the capsule (Fig. 91.2C). Open this superiorly.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


