Answer: (A) Entry of cystic duct into the common hepatic duct
Rationale:
The common hepatic duct and cystic duct join to form the common bile duct, although approximately 15% to 20% of patients will have a variation in their biliary duct anatomy. One of the more important variations to be aware of during a cholecystectomy is a short cystic duct, which leads to the common bile duct being mistaken for the cystic duct. Another variant to be cautious of during a cholecystectomy is the presence of an anterior or posterior right hepatic duct that independently inserts into the common hepatic duct. In this situation, the anterior or posterior right hepatic duct may be mistaken for the cystic duct and inadvertently clipped. The wide variation in extrahepatic biliary anatomy creates the need to establish the “critical view” during a cholecystectomy. To obtain this view, the window between the cystic duct, the inferior liver edge, and the common hepatic duct is opened so that the cystic duct and cystic artery can be identified as the only structures entering directly into the gallbladder.
References:
Jackson PG, Evans SRT. Biliary system. In: Towsend CM, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 19th ed. Philadelphia, PA: Saunders Elsevier; 2012:1476-1495.
A 55-year-old female presents with complaints of worsening chest pain associated with swallowing and dysphagia for solid food. Upper gastrointestinal series demonstrates narrowing of the distal esophagus with proximal dilation. Manometric studies demonstrate failure of normal relaxation of the lower esophageal sphincter. The patient undergoes an uneventful laparoscopic Heller myotomy. Postoperatively she reports continued chest pain that occurs 30 to 60 minutes after meals and worsens upon lying down. How could this complication have been prevented?
Combining myotomy with a partial fundoplication procedure
Esophagectomy
Injection of the lower esophageal sphincter with botulinum toxin
Longer myotomy incision
Postoperative initiation of calcium channel blockers
Answer: (A) Combining myotomy with a partial fundoplication procedure
Rationale:
Achalasia results from a progressive neuronal degeneration of Auerbach plexus within the muscular wall of the esophagus. The disease is characterized by failure of relaxation of the lower esophageal sphincter. Patients present with symptoms of dysphagia to liquids and solids and can also have regurgitation.
Initial therapy is medical, utilizing calcium channel blockers and nitrates to induce relaxation of the lower esophageal sphincter. Initial invasive management methods include pneumatic or mechanical dilation, which is associated with a risk of perforation and often requires repeat procedures for improved efficacy. Botulinum toxin injection is also used and acts by inhibiting release of excitatory acetylcholine. If medical therapy fails, surgical management is indicated.
Surgical treatment of achalasia is most commonly with a Heller esophagomyotomy, during which an anterior longitudinal incision is made within the longitudinal and circular muscle layers of the esophagus and continued onto the proximal stomach. Following this step, the lower esophageal sphincter is no longer competent, and the patient loses the ability to prevent reflux of gastric acid into the esophagus. Addition of an antireflux procedure in the form of a partial fundoplication is commonly performed and can create a mechanical barrier and decreases symptoms of gastroesophageal reflux.
Esophagectomy is considered a therapy of last resort for achalasia in patients with a severely tortuous sigmoid esophagus or those who have had failure of prior myotomy to relieve dysphagia.
Richards WO, Williams DB. Current treatment of achalasia. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Saunders Elsevier; 2011:41-45.
2G03
Key word: Diagnosis of Duodenal Stump Leak
Author: Jens U. Berli, MD
Editor: Christopher L. Wolfgang, MD, PhD
A 43-year-old female patient is now postoperative day 8 after a distal gastrectomy and Roux-en-Y reconstruction for an antral gastrointestinal stromal tumor (GIST). On morning rounds, her abdomen is tender with guarding in her epigastrium, and there is bilious fluid in her intra-abdominal Jackson-Pratt drain. Her vital signs are 38.1°C, pulse 98 beats per minute, blood pressure 123/69 mm Hg, and oxygen saturation 94%. A computed tomography (CT) scan with oral contrast is performed, and a fluid collection measuring 10 × 8 × 5 cm is seen in the area of the resection bed. Which of the following is the next step in diagnosing a duodenal stump leak?
Diagnostic laparoscopy
Fluoroscopy (upper gastrointestinal series with Jackson-Pratt injection)
Gastroscopy and inspection of anastomosis
No further studies are needed as bilious fluid in the Jackson-Pratt drain is diagnostic
Answer: (D) No further studies are needed as bilious fluid in the Jackson-Pratt drain is diagnostic
Rationale:
Duodenal stump insufficiency is a feared complication after any surgery that leaves the duodenum disconnected from the stomach (e.g., Billroth II, Whipple with side-to-end anastomosis of pancreas and duodenum, Roux-en-Y reconstruction after gastrectomy, duodenal switch). In this case, a CT scan with oral contrast has already established that an anastomotic leak has occurred, and bile in the Jackson-Pratt drain indicates that the source of this leak is the duodenum. Fluoroscopy could be used as a confirmatory test but is not required for diagnosis. Repeat CT scan is not likely to help clarify the source of the leak. Gastroscopy and inspection of the anastomosis carries the risk of worsening a potential anastomotic leak or creating one de novo. Gastroscopy is usually the preferred diagnostic and treatment tool for suspected hemorrhage of the gastrojejunal anastomosis (e.g., anastomotic ulcer).
Duodenal stump insufficiency is generally managed conservatively with drainage. In cases of high output leaks, percutaneous biliary drainage might be indicated. Diagnostic laparoscopy on postoperative day 8 is likely to be complicated by adhesions and may create additional harm. Unless appropriate drainage cannot be achieved by percutaneous drain placement, surgery should not be the first choice in management. If this were to occur on postoperative day 1, however, one might consider taking the patient back for exploration. In cases of open repair, a duodenostomy tube with or without T-tube drainage of the common bile duct can be performed with repair of the leak.
References:
Mercer DW, Robinson EK. Stomach. In: Townsend CM, Beauchamp RD, Evers MB, Mattox KL, eds. Sabiston Textbook of Surgery: the biological basis of modern surgical practice. 18th ed. Philadelphia, PA: Saunders Elsevier; 2008:1245-1275.
Richards WO, Schirmer BD. Morbid obesity. In: Townsend CM, Beauchamp RD, Evers MB, Mattox KL, eds. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 18th ed. Philadelphia, PA: Saunders Elsevier; 2008:399-429.
2G04
Key word: Diagnostic Test of Pleural Effusion after Laparoscopic Nissen Fundoplication
Author: Betsy King, MD
Editor: Robert A. Meguid, MD, MPH
A 54-year-old male undergoes laparoscopic Nissen fundoplication for persistent gastroesophageal reflux. On postoperative day 2 the patient develops pleuritic chest pain and shortness of breath. EKG and cardiac enzymes are normal. Chest x-ray demonstrates a large left-sided pleural effusion. Which of the following is the best diagnostic study to obtain next?
A rare yet serious postoperative complication of laparoscopic Nissen fundoplication is esophageal or gastric perforation secondary to injuries caused by surgical instrumentation of the viscera. A perforation presents most commonly within the first 48 hours after surgery, and risk is increased if there is any postoperative retching or emesis.
Perforation often presents with peritoneal signs if leakage of gastrointestinal contents is contained within the abdomen. Dyspnea and pleural effusion are common symptoms and are signs of a leak into the chest. Barium or water-soluble contrast swallow study will definitively diagnose the leak and may also identify the site of perforation. Definitive management is by exploratory laparotomy and direct surgical repair of the defect.
CT scan is a reasonable diagnostic study to evaluate the nature of the chest x-ray findings but is not sensitive in identifying visceral perforations because it is not a dynamic study. It may identify stigmata associated with perforation such as pneumoperitoneum (often present for several days after a laparoscopic procedure) or a large effusion. Sampling the pleural effusion would give more information regarding the composition of the effusion; however, it would neither provide a definitive diagnosis nor identify the site of perforation. Lymphoscintigraphy would be useful in the diagnosis of chylous effusion secondary to thoracic duct injury in the setting of a large chyle leak. While the thoracic duct does run alongside the esophagus, injury to it is rare during laparoscopic Nissen fundoplication.
Maish M. Esophagus. In: Towsend CM, Beuchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 18th ed. Philadelphia, PA: Saunders Elsevier; 2008.
2G05
Key word: Diagnosis of VIPoma
Author: Ibrahim Sultan, MD
Editor: Richard D. Schulick, MD, MBA, FACS
A 52-year-old man presents to the emergency room with abdominal pain, weight loss, and dehydration. He has had largevolume diarrhea (>3 L/day) over the past few weeks. Abdominal computed tomography (CT) reveals a small mass in the tail of the pancreas, and a plasma vasoactive intestinal polypeptide (VIP) is sent. Which of the following would be most consistent with a diagnosis of Verner-Morrison syndrome?
A VIP level greater than 75 pg/mL in a patient with largevolume diarrhea and a pancreatic mass is highly suggestive of VIPoma or Verner-Morrison syndrome. The diagnostic triad for a VIPoma is secretory diarrhea, high plasma VIP levels, and a pancreatic tumor. Patients with low-volume diarrhea (<700 mL/day) are unlikely to have a VIPoma. Weight loss and abdominal pain are both nonspecific findings that are not necessarily present in a patient with a VIPoma.
VIPoma is a quite rare tumor, and patients commonly present with severe electrolyte disturbances (the syndrome is also known as watery diarrhea, hypokalemia, and achlorhydria syndrome [WDHA] syndrome). Stool osmotic gap in patients with VIPoma is usually <50 mOsm/kg, reflecting a secretory diarrhea. A stool osmotic gap of >125 mOsm/kg suggests an osmotic diarrhea (e.g., from ingestion of laxatives or excessive sugar or salt).
Diagnosis Vipoma
Parameter
Description
Symptoms Watery diarrhea
Weakness
Lethargy
Nausea
Diagnostic tests
Hypokalemia
Achlorhydria
Metabolic acidosis
Serum VIP levels elevated
Anatomic localization
Most in body and tail of pancreas, with liver metastases
Kennedy EP, Brody JR, Yeo CJ. Neoplasms of the endocrine pancreas. In: Mulholland MW, Lillemoe KD, Doherty GM, Maier RV, Upchurch GR, eds. Greenfield’s Surgery: Scientific Principles & Practice. 5th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2011.
Ladner D, Norton JA. Neuroendocrine tumors of the pancreas. In: Yeo CJ, ed. Shackelford’s Surgery of the Alimentary Tract. 6th ed. Philadelphia, PA: Elsevier; 2007:1375-1386.
Key word: Etiology of Increased Enzymes with Common Bile Duct Injury
Author: Andrew P. Dhanasopon, MD
Editor: Christopher L. Wolfgang, MD, PhD
A 45-year-old woman undergoes a laparoscopic cholecystectomy for symptomatic cholelithiasis. On postoperative day 10, she presents to the emergency room with 4 days of lowgrade fevers, nausea, and right upper quadrant abdominal pain. Laboratory studies reveal mildly elevated bilirubin, liver enzymes, and white blood cell count. Computed tomography demonstrates a subhepatic fluid collection. Hepatobiliary iminodiacetic acid (HIDA) scan shows some drainage enterically but also peritoneal leakage, and a percutaneous drain is placed into the collection. What is the next step in management?
Endoscopic retrograde cholangiopancreatography (ERCP) with stenting
Answer: (A) Endoscopic retrograde cholangiopancreatography (ERCP) with stenting
Rationale:
A bile duct injury cannot be treated with observation alone. Identification of the site of injury is the key at this step in management. A percutaneous transhepatic cholangiogram will allow for identification of the site of leakage, but ERCP is both a diagnostic and therapeutic modality and is therefore the better choice. Immediate open surgery is not indicated until the site and extent of biliary injury has been determined. If bile duct injury is recognized after the first week, hepaticojejunostomy is generally not recommended.
References:
Connor S, Garden OJ. Bile duct injury in the era of laparoscopic cholecystectomy. Br J Surg. 2006;93(2):158-168.
Rauws EAJ, Gouma DJ. Endoscopic and surgical management of bile duct injury after laparoscopic cholecystectomy. Best Pract Res Clin Gastroenterol. 2004;18(5):829-846.
2G07
Key word: Evaluation of Foregut Symptoms
Author: Betsy King, MD
Editor: Richard D. Schulick, MD, MBA, FACS
A 56-year-old male with a significant history of tobacco use complains of progressively worsening odynophagia and dysphagia and a 4.5-kg (10-lb) weight loss over the past several months. He initially had trouble swallowing solid food and has more recently developed difficulty swallowing liquids and a sensation that food gets caught in his chest. What is the most valuable diagnostic study to obtain?
The differential diagnosis for dysphagia includes benign etiologies such as achalasia as well as malignant etiologies such as esophageal cancer. The history of tobacco use and weight loss in this patient should signal a red flag that cancer must be ruled out. Although all of the choices are acceptable means of evaluating esophageal pathology, esophagogastroduodenoscopy is the most valuable in establishing a diagnosis. Endoscopy allows for direct visualization of the esophagus and for collection of biopsies.
Fluoroscopic imaging, such as barium swallow, is useful for evaluating esophageal function and giving a gross representation of the mucosal surface. It is useful for identifying certain motility disorders and gastroesophageal reflux but provides limited information regarding the diagnosis of cancer. Likewise, CT is useful in examining extraluminal esophageal disease that can often be present with esophageal carcinoma. However, cross-sectional imaging does not provide evaluation of the mucosal surface where most cancers originate.
Endoscopic ultrasound is very sensitive for determining the depth of invasion of a known cancer, but it is not typically used as the initial diagnostic assessment. Endoscopic ultrasound can also be utilized for fine-needle aspiration and lymph node sampling. Esophageal manometry is generally reserved for evaluation of esophageal pathology once a structural etiology has been ruled out. It is the preferred diagnostic study for disorders of esophageal motility.
Chandrasekhara V, Jagannath S. Esophageal function tests. In: Cameron JL, Cameron AL, eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Saunders Elsevier; 2011:1-14.
2G08
Key word: Initial Treatment of Diverticular Disease
Author: Ibrahim Sultan, MD
Editor: Susan L. Gearhart, MD
A 50-year-old man presents to the emergency room with left lower quadrant abdominal pain. He is febrile to 38.7°C with a pulse of 100 beats per minute and blood pressure of 120/70 mm Hg. On examination of his abdomen, he is found to have focal left lower quadrant tenderness without peritonitis. His white blood cell count is 15,000/µL, and a computed tomography (CT) scan demonstrates diverticular disease in the sigmoid colon with a 6-cm rim-enhancing pericolic collection. Antibiotics are started. What is the next step in management of this patient?
Careful observation on antibiotic therapy
Exploratory laparotomy and washout without operative resection of the colon
Percutaneous drainage of the collection
Sigmoid colectomy with end colostomy and Hartmann pouch
Answer: (C) Percutaneous drainage of the collection
Rationale:
This patient presents with complicated diverticulitis, that is, diverticular disease with abscess, perforation, stricture, or fistulous disease. Uncomplicated disease involves abdominal pain, fever, leukocytosis, and obstipation in the absence of the complications noted for complicated disease.
Complicated diverticular disease is further classified according to the Hinchey classification. Stage 1 involves a pericolic or intramesenteric abscess. Stage 2 presents with a pelvic abscess. Stage 3 presents with generalized purulent peritonitis without gross intestinal perforation. Stage 4 presents with fecal peritonitis.
The initial management of stage 1 disease in the absence of peritonitis or hemodynamic instability consists of percutaneous drainage and intravenous antibiotics. If operative management is pursued, the choice of operation would be sigmoid resection with primary anastomosis. The anastomotic leak rate is approximately 4% in this setting, and a diverting ostomy is not recommended.
Reference:
Gearhart SG. Diverticular disease of the colon. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Elsevier; 2010:132-136.
2G09
Key word: Initial Treatment of Appendiceal Abscess
Author: Vicente Valero III, MD
Editor: Mark D. Duncan, MD, FACS
A 26-year-old man with no significant past medical history arrives to the emergency department complaining of right lower quadrant pain. His pain initially began in the periumbilical region, and he ignored the pain for the last 48 hours. His temperature is 39°C and his white blood cell count is 16,000/µL. Computed tomography (CT) scan of the abdomen and pelvis shows a 6- × 8-cm rim-enhancing fluid collection in the right pelvis. What is the best next step in the management of this patient’s disease?
Admission to the surgical ward, intravenous antibiotics, and laparoscopic appendectomy during this hospitalization
Admission to the surgical ward, intravenous antibiotics, and repeat CT of the abdomen and pelvis in 5 days
Admission to the surgical ward, intravenous antibiotics, percutaneous drainage of the fluid collection, and interval appendectomy
Discharge patient on oral antibiotics
Discharge patient on oral antibiotics and then perform interval appendectomy
Answer: (C) Admission to the surgical ward, intravenous antibiotics, percutaneous drainage of the fluid collection, and interval appendectomy
Rationale:
Perforated appendicitis is a common complication due to delayed presentation or erroneous diagnosis. Usually the inflammatory process has been present for 5 to 7 days before rupture. The overall incidence of appendiceal perforation is about 25%. Rupture is more common in the extremes of age, occurring more frequently in children younger than 5 years of age and adults older than 65 years of age. Patients typically present with localized peritonitis, as the omentum and bowels wall off the abscess preventing generalized peritonitis in most patients.
Patients with appendiceal abscess should be admitted to the surgical ward and administered intravenous antibiotics. An interventional radiology consult should be obtained for percutaneous drainage of the collection. Intravenous antibiotics should be continued for several days and then the patient can be transitioned to an oral regimen and discharged from the hospital. Definitive management with removal of the appendix should be undertaken with an elective laparoscopic appendectomy performed around 6 weeks from initial presentation.
Reference:
Jaffe BM, Berger DH. The appendix. In: Brunicardi FC, Brandt ML, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE, eds. Schwartz’s Principles of Surgery. 9th ed. New York, NY: McGraw-Hill; 2010:1119-1137.
2G10
Key word: Initial Treatment of Echinococcal Liver Cyst
Author: Bonnie E. Lonze, MD, PhD
Editor: Michael A Choti, MD, MBA
A 22-year-old male college student presents with anorexia and vague abdominal pain 6 months after returning from a semester abroad in Argentina. A computed tomography (CT) scan of his abdomen reveals a 10-cm, thick-walled cystic lesion and several smaller neighboring cysts. He is afebrile, has a normal white blood cell count, and normal total bilirubin. This patient is most appropriately managed with:
Immediate surgical resection followed by albendazole
Immediate surgical resection followed by metronidazole
Medical monotherapy with metronidazole
Preoperative albendazole followed by surgical therapy
Preoperative metronidazole followed by surgical resection
Answer: (D) Preoperative albendazole followed by surgical therapy
Rationale:
Hydatid cysts of the liver develop as a consequence of infection with the tapeworm Echinococcus, a parasite endemic to regions of South America, Central Asia, and the Mediterranean. Dogs are carriers of the parasite, and sheep and goats are intermediate hosts. Ingestion of contaminated food products or contact with infected animals can lead to human infection. After ingestion of eggs, parasitic embryos circulate and lead to formation of hydatid cysts, most commonly in the liver.
Ultrasound and CT scanning are the most useful imaging studies for establishing a diagnosis of hydatid cysts of the liver. Hydatid cysts classically are large lesions with thick and often calcified walls. Daughter cysts, which appear as neighboring smaller cystic lesions, may also be evident. Infection with the species Echinococcus multilocularis can produce a picture of multiple small cysts.
Surgery is the primary treatment for hydatid cysts, although the antihelminthic agent albendazole should be administered preoperatively as an adjunct. Albendazole has been found to accumulate in cysts at higher concentrations than mebendazole and is therefore the first-line medical therapy. Medical therapy alone is used only for patients who are particularly poor operative candidates. The goal of surgical therapy is to remove the viable cyst components without spillage of cyst contents. The extent of operation required ranges from cystectomy to partial hepatectomy to even liver transplantation in rare circumstances. Endoscopic retrograde cholangiopancreatography (ERCP) should be performed preoperatively to evaluate for cyst communication with the biliary tree to assist in determination of the extent of necessary liver resection.
Reference:
Hong JC. Echinococcal disease of the liver. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Mosby; 2011:276-281.
2G11
Key word: Initial Treatment for Respiratory Complications with Pancreatic Ascites
Author: Jens U. Berli, MD
Editor: Christopher L. Wolfgang, MD, PhD
A 51-year-old male with a history of chronic pancreatitis and pseudocysts presents to the emergency room with subjective dyspnea and ascites. His ascitic fluid has an amylase value of 2,476 Units/L. The patient is admitted and managed nonoperatively. Despite these measures, he develops increasing respiratory symptoms. You relieve his immediate symptoms with a bedside thoracentesis. Which next step in management is most appropriate?
Drain placement by interventional radiology
Endoscopic retrograde cholangiopancreatography (ERCP) with pancreatic stent placement
Answer: (B) Endoscopic retrograde cholangiopancreatography (ERCP) with pancreatic stent placement
Rationale:
Pancreatic ascites is most commonly due to pancreatic duct disruption (e.g., traumatic injury, ruptured pseudocyst, iatrogenic injury). The patient above has a history of chronic pancreatitis with formation of pseudocysts. Most likely a pseudocyst has ruptured, exposing an ongoing leakage from a pancreatic duct. Conservative measures (nothing by mouth, nasogastric decompression, and octreotide administration) lead to resolution in 40% to 60% of patients. Should this management fail (as in this patient), more invasive methods are then used that aim to decrease the rate of the leakage. An ERCP with stent placement and papillotomy is the least invasive method and also gives diagnostic opportunity to localize the exact area of extravasation. A Whipple or a distal pancreatectomy is the most invasive choice if other methods fail.
Other causes of ascites such as malignancy or liver disease have to be excluded prior to any interventions. Transjugular portosystemic shunt would not help this patient since the etiology of his ascites is not portal hypertension. Endoscopic gastrocystostomy is not a therapy of choice for a cyst that has already ruptured.
Reference:
Steer ML. Exocrine pancreas. In: Townsend CM, Beauchamp RD, Evers MB, Mattox KL, eds. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 18th ed. Philadelphia, PA: Saunders Elsevier; 2008:1605-1606.
2G12
Key word: Procedure with the Greatest Risk of Postoperative Small Bowel Obstruction
Author: Betsy King, MD
Editor: Susan L. Gearhart, MD
A 65-year-old man presents to the emergency room with bilious vomiting and abdominal pain. He is of status post a sigmoidectomy 6 weeks ago for diverticular disease. He is afebrile, pulse is 110 beats per minute, and blood pressure is 120/70 mm Hg. Which of the following is the most likely cause for his symptoms?
The most likely cause for this patient’s presentation is small bowel obstruction. The leading cause of small bowel obstruction in the United States is surgical adhesions. This patient underwent abdominal surgery 6 weeks prior to presentation and is at risk of developing postoperative adhesions. In the United States, nearly 90% of all small bowel obstructions occur in patients with history of prior surgery secondary to the development of surgical adhesions. Postoperative small bowel obstruction is more likely to occur greater than 30 days following the surgery, when there has been sufficient time for scar formation. Furthermore, adhesions are more likely to form in the setting of active inflammation such as inflammatory bowel disease, diverticulitis, or operations involving penetrating abdominal trauma with contamination.
The patient above has no symptoms of active inflammation making recurrent diverticular disease, urinary tract infection, or bowel perforation less likely. An anastomotic leak would be expected much earlier in the patient’s postoperative course, and by 6 weeks the anastomosis should be well healed.
Stewart RM, Page CP, Brender J, et al. The incidence and risk of early postoperative small bowel obstruction. A cohort study. Am J Surg. 1987;154:643-647.
2G13
Key word: Risk of Rebleeding of Duodenal Ulcer
Author: Kyle J. Van Arendonk, MD, PhD
Editor: Pamela A. Lipsett, MD, MHPE, FACS, FCCM
A 65-year-old man presents with hematemesis. He is resuscitated and started on a pantoprazole infusion. Upper endoscopy identifies a posterior duodenal ulcer with a nonbleeding visible vessel that is coagulated and clipped. Which of the following is true regarding the potential for rebleeding in this duodenal ulcer?
An episode of rebleeding after endoscopic treatment mandates surgical exploration
Continuation of the intravenous proton pump inhibitor after endoscopic therapy is unnecessary
The posterior location of the ulcer is associated with a lower risk of rebleeding
The presence of a nonbleeding visible vessel is associated with a higher risk of rebleeding than an adherent clot
Answer: (D) The presence of a nonbleeding visible vessel is associated with a higher risk of rebleeding than an adherent clot
Rationale:
Hemodynamically stable patients with upper gastrointestinal bleeding should undergo upper endoscopy after appropriate resuscitation. The endoscopic findings can then be used to predict the likelihood of recurrent hemorrhage and guide management decisions. Specifically, these so-called “stigmata of recent hemorrhage” include the following potential appearances of the ulcer base, in descending risk of rebleeding: Active spurting, nonbleeding visible vessel, active oozing, adherent clot, flat pigmented spot, and clean base.
In addition to these stigmata seen on endoscopy, increased patient age, anemia at presentation, hypovolemic shock, the need for blood transfusion, posterior location of the ulcer, and significant comorbidities, in particular hepatic or renal failure or metastatic cancer, are also associated with an increased risk of recurrent bleeding.
Successful endoscopic hemostasis in patients with highrisk stigmata should be followed with continuation of intravenous proton pump inhibitor in order to decrease the risk of further bleeding. In patients who do develop signs of rebleeding, repeat endoscopy with additional endoscopic therapy can still be performed, as most patients with recurrent bleeding will be able to avoid surgery via successful repeat endoscopic therapy. If rebleeding occurs again after a second endoscopic treatment, the patient should proceed to surgery or arterial embolization by interventional radiology.
References:
Laine L, Jensen DM. Management of patients with ulcer bleeding. Am J Gastroenterol. 2012;107(3):345-360.
Key word: Treatment of Adenocarcinoma of the Appendix
Author: Ibrahim Sultan, MD
Editor: Jonathan E. Efron, MD
A 37-year-old man undergoes a laparoscopic appendectomy for presumed appendicitis and is discharged home without any complications. Pathologic examination reveals a 1-cm adenocarcinoma of the tip of the appendix that is margin negative. What is the next step in management?
Chemotherapy
Close surveillance with computed tomography scan in 6 months
No further therapy
Positron emission tomography scan to evaluate for residual disease
Appendiceal tumors are found in approximately 1% of pathologic specimens. Most of these tumors are carcinoid tumors, which typically arise from the tip of the appendix. Carcinoid tumors that are less than 1 cm in size and do not involve the base are managed only with an appendectomy. Carcinoid tumors that are greater than 2 cm in size are managed with a right hemicolectomy. However, the optimal management of all adenocarcinomas of the appendix involves a right hemicolectomy to remove the lymph node drainage of the appendix along the ileocolic mesentery.
References:
Compton C, Hawk E, Grochow L, et al. Colon cancer. In: Abeloff MD, Armitage JO, Niederhuber JE, Kastan MB, McKenna WG. Abeloff’s Clinical Oncology. 4th ed. Philadelphia, PA: Churchill Livingstone Elsevier; 2008: 1477-1524.
Sugarbaker PH. Cancer of the appendix and pseudomyxoma peritonei syndrome. In: Fazio VW, Church JM, Delaney CP, eds. Current Therapy in Colon and Rectal Surgery. 2nd ed. Philadelphia, PA: Elsevier; 2005:369-378.
2G15
Key word: Treatment of Amebic Liver Abscess
Author: Bonnie E. Lonze, MD, PhD
Editor: Michael A. Choti, MD, MBA
A 29-year-old surgery resident presents with anorexia, weight loss, and right upper quadrant pain. A month ago, she returned from a 1-year medical mission to Mexico. Shortly after she had arrived in Mexico, she had a brief bout of self-limited diarrhea but otherwise remained in good health for the duration of the trip. A computed tomography (CT) scan of the abdomen reveals a right-sided intrahepatic rim-enhancing fluid-filled lesion. The first-line treatment option for this patient is:
Intravenous metronidazole
Intravenous praziquantel
Intravenous praziquantel followed by percutaneous drainage
Amebic hepatic abscesses are caused by infection with the protozoan Entamoeba histolytica. Infection is transmitted by the fecal-oral route, and typically initial infection leads to a diarrheal disease referred to as amebic dysentery. While the liver is the most common site of extra-intestinal infection, only a small percentage of patients develop hepatic abscesses, which typically present in a delayed fashion following amebic dysentery.
Amebic abscesses are almost always successfully treated with metronidazole, which is able to achieve high concentrations in the liver. Drainage by any route, percutaneous or open, is almost never required. Paromomycin is a luminal antimicrobial that is administered to eradicate the amoeba from the intestinal tract. It is often administered in conjunction with metronidazole to prevent recurrence of hepatic abscesses but is not by itself an appropriate therapy for treatment of the extraintestinal amebic diseases. Praziquantel is an antihelminthic agent used for the treatment of schistosomiasis and is ineffective in the treatment of amebic abscesses.
References:
Edil B, Pitt H. Hepatic abscess. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Mosby; 2011:301-305.
Subramanian A, Gurakar A, Klein A, et al. Hepatic infection and acute hepatic failure. In: Mulholland MW, Lillemoe KD, Doherty GM, Maier RV, Upchurch GR, eds. Greenfield’s Surgery: Scientific Principles & Practice. 5th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2011.
Figure
Sonogram (A) and computed tomogram (B) in a patient with multiple amebic abscesses (arrows). Reprinted with permission from: Subramanian A, Gurakar A, Klein A, et al. Hepatic infection and acute hepatic failure. In: Mulholland MW, Lillemoe KD, Doherty GM, Maier RV, Upchurch GR, eds. Greenfield’s Surgery: Scientific Principles & Practice. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:890.
2G16
Key word: Treatment of Autoimmune Pancreatitis
Author: Ibrahim Sultan, MD
Editor: Richard D. Schulick, MD, MBA, FACS
A 57-year-old man with a history of psoriasis presents to the hospital with signs and symptoms of acute pancreatitis. Computed tomography (CT) shows diffuse enlargement of the pancreas. The pancreatic duct appears to be diminutive. He has elevated levels of IgG4 and after ruling out malignancy with endoscopic ultrasound and biopsy, a diagnosis of autoimmune pancreatitis is made. What is the next step in management of this patient?
Autoimmune pancreatitis is a form of chronic pancreatitis characterized by a mixed inflammatory infiltrate with prominent lymphocytic infiltration. The inflammatory process centers on the pancreatic duct, causing pancreatic duct stenosis. The resulting fibrosis of the pancreas causes organ dysfunction. Some patients will have other associated autoimmune conditions such as Sjögren syndrome, psoriasis, primary sclerosing cholangitis, or inflammatory bowel disease.
Autoimmune pancreatitis can be difficult to differentiate from pancreatic adenocarcinoma. Patients can present with a pancreatic mass and may need additional workup such as an endoscopic ultrasound with biopsy or rather a laparoscopic or open biopsy in order to rule out malignancy. A serum IgG4 level greater than 140 mg/dL is highly suggestive of autoimmune pancreatitis but cannot definitely rule out pancreatic cancer.
Autoimmune pancreatitis is initially managed medically with steroids (prednisone 30 to 40 mg/day) for approximately 4 to 6 weeks. Patients typically respond in 2 to 4 weeks. If there is no response to steroids, an alternative diagnosis should always be considered.
References:
Krasinskas AM, Raina A, Khalid A, et al. Autoimmune pancreatitis. Gastroenterology Clin North Am. 2007;36(2):239-257.
Vollmer CM, Kent TS, Callery MP. Unusual pancreatic tumors. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Elsevier; 2010:444-449.
2G17
Key word: Treatment of Tracheoneoesophageal Fistula after Esophagectomy
Author: Jens U. Berli, MD
Editor: Robert A. Meguid, MD, MPH
A 64-year-old woman who is postoperative day 23 status post Ivor Lewis esophagectomy for esophagogastric junction cancer is readmitted to the surgical intensive care unit with fever, hypotension, and a productive cough. She is resuscitated with fluid and started on broad-spectrum antibiotics. Chest x-ray demonstrates right lower lobe consolidation but no pleural fluid collection. Esophagogram reveals a small tracheo-neoesophageal fistula at the level of the esophagogastric anastomosis. The patient is made NPO and total parenteral nutrition (TPN) is initiated. Which of the following is the most appropriate next step in management of this complication?
Primary surgical repair
Reintubation
Tracheal ring resection
Tracheal stent
Video-assisted thoracoscopic decortication and tube thoracostomy placement
Tracheo-neoesophageal fistulas are a dreaded complication after esophagectomy occurring in approximately 3% to 4% of cases. Most often this is an early complication, but it can also occur several years after the operation. The injury can result from endotracheal tube pressure, anastomotic leak, chronic reflux, or ischemic lesions due to mediastinal devascularization or radiation. The principles of treatment are drainage of any fluid collections that may represent leakage of enteric contents, control of ongoing leakage, and definitive repair.
The approach to this complication depends on the clinical scenario. Any intra-abdominal or intrathoracic collections must be drained. If the fistula is discovered in the early postoperative period (the first few days after surgery) and the patient is not critically ill, return to the operating room for a primary repair may be attempted. Operative repair consists of resection of the fistula with primary repair of the trachea and neoesophagus conduit along with a muscular flap to separate the two suture lines. If the patient has a larger defect or is critically ill, a tracheal stent is the initial therapy of choice. This strategy allows for source control of ongoing leak and gives the patient time to recover from infection. The patient should remain on TPN or postpyloric alimentation. Should a small fistula fail to heal after stent placement, the patient is brought back to the operating room once clinically stable for definite repair of the fistula and muscle flap coverage.
Tube thoracostomy placement is necessary for drainage of enteric contents that are present at the time of diagnosis, and thoracoscopic or open decortication may be necessary if a rind has already developed on the lung or infection does not resolve with thoracostomy drainage. Reintubation with placement of the tracheal cuff distal to the fistula might be necessary in the case of pulmonary failure.
Only gold members can continue reading. Log In or Register to continue
 Entry of cystic duct into the common hepatic duct
Entry of cystic duct into the common hepatic duct Entry of the duct into the pancreas
Entry of the duct into the pancreas The change in mucosa from columnar to squamous
The change in mucosa from columnar to squamous The intersection of the bile duct and right hepatic artery
The intersection of the bile duct and right hepatic artery The superior edge of the duodenum where the duct starts to travel in the retroduodenal space
The superior edge of the duodenum where the duct starts to travel in the retroduodenal space Combining myotomy with a partial fundoplication procedure
Combining myotomy with a partial fundoplication procedure Esophagectomy
Esophagectomy Injection of the lower esophageal sphincter with botulinum toxin
Injection of the lower esophageal sphincter with botulinum toxin Longer myotomy incision
Longer myotomy incision Postoperative initiation of calcium channel blockers
Postoperative initiation of calcium channel blockers Diagnostic laparoscopy
Diagnostic laparoscopy Fluoroscopy (upper gastrointestinal series with Jackson-Pratt injection)
Fluoroscopy (upper gastrointestinal series with Jackson-Pratt injection) Gastroscopy and inspection of anastomosis
Gastroscopy and inspection of anastomosis No further studies are needed as bilious fluid in the Jackson-Pratt drain is diagnostic
No further studies are needed as bilious fluid in the Jackson-Pratt drain is diagnostic Repeat CT scan with oral and intravenous contrast
Repeat CT scan with oral and intravenous contrast Computed tomography (CT) scan
Computed tomography (CT) scan Echocardiogram
Echocardiogram Esophagogram
Esophagogram Lymphoscintigraphy
Lymphoscintigraphy Thoracentesis and pleural fluid sampling
Thoracentesis and pleural fluid sampling Abdominal pain
Abdominal pain Osmotic diarrhea
Osmotic diarrhea Stool osmotic gap of 300 mOsm/kg
Stool osmotic gap of 300 mOsm/kg VIP plasma level of 600 pg/mL
VIP plasma level of 600 pg/mL Weight loss
Weight loss Endoscopic retrograde cholangiopancreatography (ERCP) with stenting
Endoscopic retrograde cholangiopancreatography (ERCP) with stenting Immediate open common bile duct exploration
Immediate open common bile duct exploration Immediate open hepaticojejunostomy
Immediate open hepaticojejunostomy Observation
Observation Percutaneous transhepatic cholangiogram
Percutaneous transhepatic cholangiogram Barium swallow
Barium swallow Computed tomography (CT) of the chest and abdomen
Computed tomography (CT) of the chest and abdomen Endoscopic ultrasound
Endoscopic ultrasound Esophageal manometry
Esophageal manometry Esophagogastroduodenoscopy
Esophagogastroduodenoscopy Careful observation on antibiotic therapy
Careful observation on antibiotic therapy Exploratory laparotomy and washout without operative resection of the colon
Exploratory laparotomy and washout without operative resection of the colon Percutaneous drainage of the collection
Percutaneous drainage of the collection Sigmoid colectomy with end colostomy and Hartmann pouch
Sigmoid colectomy with end colostomy and Hartmann pouch Sigmoid colectomy with primary anastomosis
Sigmoid colectomy with primary anastomosis Admission to the surgical ward, intravenous antibiotics, and laparoscopic appendectomy during this hospitalization
Admission to the surgical ward, intravenous antibiotics, and laparoscopic appendectomy during this hospitalization Admission to the surgical ward, intravenous antibiotics, and repeat CT of the abdomen and pelvis in 5 days
Admission to the surgical ward, intravenous antibiotics, and repeat CT of the abdomen and pelvis in 5 days Admission to the surgical ward, intravenous antibiotics, percutaneous drainage of the fluid collection, and interval appendectomy
Admission to the surgical ward, intravenous antibiotics, percutaneous drainage of the fluid collection, and interval appendectomy Discharge patient on oral antibiotics
Discharge patient on oral antibiotics Discharge patient on oral antibiotics and then perform interval appendectomy
Discharge patient on oral antibiotics and then perform interval appendectomy Immediate surgical resection followed by albendazole
Immediate surgical resection followed by albendazole Immediate surgical resection followed by metronidazole
Immediate surgical resection followed by metronidazole Medical monotherapy with metronidazole
Medical monotherapy with metronidazole Preoperative albendazole followed by surgical therapy
Preoperative albendazole followed by surgical therapy Preoperative metronidazole followed by surgical resection
Preoperative metronidazole followed by surgical resection Drain placement by interventional radiology
Drain placement by interventional radiology Endoscopic retrograde cholangiopancreatography (ERCP) with pancreatic stent placement
Endoscopic retrograde cholangiopancreatography (ERCP) with pancreatic stent placement Minilaparotomy and evacuation of the ascites
Minilaparotomy and evacuation of the ascites Transjugular portosystemic shunt
Transjugular portosystemic shunt Whipple procedure
Whipple procedure Anastomotic leak
Anastomotic leak Perforated diverticulum
Perforated diverticulum Recurrent diverticular disease
Recurrent diverticular disease Small bowel obstruction
Small bowel obstruction Urinary tract infection
Urinary tract infection An episode of rebleeding after endoscopic treatment mandates surgical exploration
An episode of rebleeding after endoscopic treatment mandates surgical exploration Continuation of the intravenous proton pump inhibitor after endoscopic therapy is unnecessary
Continuation of the intravenous proton pump inhibitor after endoscopic therapy is unnecessary The posterior location of the ulcer is associated with a lower risk of rebleeding
The posterior location of the ulcer is associated with a lower risk of rebleeding The presence of a nonbleeding visible vessel is associated with a higher risk of rebleeding than an adherent clot
The presence of a nonbleeding visible vessel is associated with a higher risk of rebleeding than an adherent clot Younger patients have a higher risk of rebleeding
Younger patients have a higher risk of rebleeding Chemotherapy
Chemotherapy Close surveillance with computed tomography scan in 6 months
Close surveillance with computed tomography scan in 6 months No further therapy
No further therapy Positron emission tomography scan to evaluate for residual disease
Positron emission tomography scan to evaluate for residual disease Right hemicolectomy
Right hemicolectomy Intravenous metronidazole
Intravenous metronidazole Intravenous praziquantel
Intravenous praziquantel Intravenous praziquantel followed by percutaneous drainage
Intravenous praziquantel followed by percutaneous drainage Oral paromomycin
Oral paromomycin Percutaneous abscess drainage
Percutaneous abscess drainage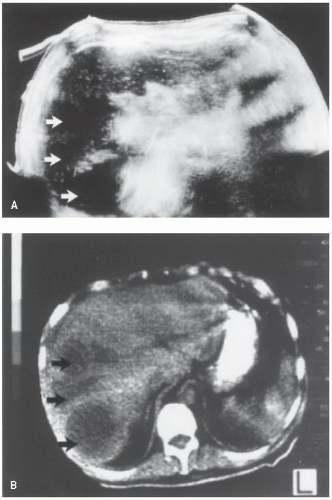
 Frey procedure
Frey procedure Glucocorticoids
Glucocorticoids Intravenous antibiotics
Intravenous antibiotics No further management
No further management Puestow procedure
Puestow procedure Primary surgical repair
Primary surgical repair Reintubation
Reintubation Tracheal ring resection
Tracheal ring resection Tracheal stent
Tracheal stent Video-assisted thoracoscopic decortication and tube thoracostomy placement
Video-assisted thoracoscopic decortication and tube thoracostomy placement


