Gastric Resection with D2 Nodal Dissection for Gastric Adenocarcinoma
Hisakazu Hoshi
As the incidence of gastric cancer declines, gastrectomy for gastric carcinoma is becoming one of the rarely performed operations for general surgeons. The extent of nodal dissection associated with the operation is a topic of debate but current national guidelines recommend resection of regional lymph nodes. This chapter reviews anatomy and technique of both distal and total gastrectomies with D2 nodal dissection. Additional material on technique of gastrectomy and BI and BII reconstructions is given in Chapter 61.
SCORE™, the Surgical Council on Resident Education, classified partial and total gastrectomies as “ESSENTIAL UNCOMMON” procedures.
STEPS IN PROCEDURE
Gastrectomy with D2 Nodal Dissection (Common Portion)
Upper midline incision and through abdominal exploration
Assess resectability, undetected metastatic disease
Retract greater omentum cephalad and detach from transverse colon, preserving mesentery to colon
Dissect infrapyloric nodal station and ligate right gastroepiploic vessels
Ligate right gastric artery and dissect suprapyloric nodal station
Divide duodenum with stapler
Divide lesser omentum to the GE junction
Dissect nodes along the hepatic artery
Elevate stomach and divide left gastric artery at its origin
Dissect celiac and proximal splenic nodal stations
Distal Gastrectomy
Dissect right paracardiac nodes and lesser curvature nodes toward resection line
Ligate left gastroepiploic vessels and dissect greater curvature nodes toward resection line
Divided stomach with 3 to 5 cm margin
Total Gastrectomy
Ligate left gastroepiploic vessels and divide gastrosplenic ligament by ligating all short gastric arteries
Isolate distal esophagus and divide
For Roux-en-Y Reconstruction
Divide upper jejunum 20 to 30 cm past ligament of Treitz
Pass jejunum to stomach or esophagus (if total gastrectomy)
Antecolic, or through hole in transverse mesocolon (retrocolic)
End-to-side esophagojejunostomy with circular staple or end-to-end gastrojejunostomy (stapled or sutured)
Jejunojejunostomy (stapled or sutured)
Side-to-side jejunojenunostomy 40 to 45 cm from anastomosis
HALLMARK ANATOMIC COMPLICATIONS
Injury to
common bile duct
celiac artery branches
portal or splenic vein
spleen
pancreas
Gastric remnant necrosis from splenic artery injury
LIST OF STRUCTURES
Esophagus
Right diaphragmatic crus
Stomach
Lesser curvature
Greater curvature
Antrum
Esophagogastric junction
Pylorus
Duodenum
Ligament of Treitz
Spleen
Transverse colon
Transverse mesocolon
Greater omentum
Lesser omentum
Lesser sac
Hepatoduodenal ligament
Middle colic vessels
Right accessory colic vein
Right gastroepiploic vein
Gastro colic trunk
Right gastroepiploic artery
Right gastric artery
Pancreas
Common bile duct
Celiac artery
Common hepatic artery
Proper hepatic artery
Splenic artery
Posterior gastric artery
Left gastric artery
Left gastric vein (coronary vein)
Left gastroepiploic artery
Portal vein
Splenic vein
Liver
Left lateral lobe of liver
Caudate lobe
Gastrosplenic ligament
Short gastric arteries
Definition of the Nodal Stations and the D1 and D2 Nodal Dissections
The nodal stations around the stomach are anatomically defined and numerically classified by the Japanese Classification of Gastric Carcinoma published by Japanese Gastric Cancer Association (JGCA) (Fig. 62.1, Table 62.1). Perigastric nodal stations are numbered 1 to 6 and regional nodal stations are 7 to 12. Nodal stations numbered higher than 12 are generally considered “distant” nodal stations and are not dissected for the standard D2 nodal dissection except nodal station 14v.
The level of the nodal dissection, known as D number, is defined by the guidelines from JGCA. While the classic D1 nodal dissection is defined by complete dissection of the first-tier nodal stations (which are determined by the location of the primary lesion and is most compatible with current concept of the “D1 nodes, perigastric nodes [stations 1 to 6]” in western literature), current (2010) definition of D1 nodal dissection in Japan includes left gastric artery node station (station 7) in addition to the perigastric nodal stations due to the observed high rate of metastasis in this nodal station by the early gastric cancer.
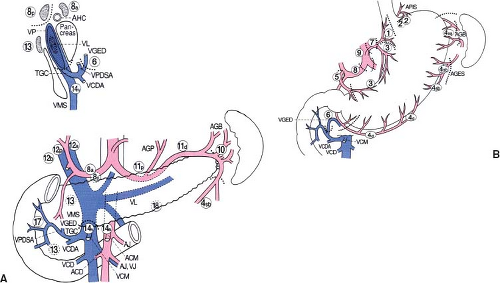 Figure 62.1 A and B: Location and border of lymph node stations by Japanese Gastric Cancer Association (from Japanese Gastric Cancer Association. Figure 7. In: Japanese Classifications of Gastric Carcinoma. 14th ed. Tokyo, Japan: Kanehara & Co. Ltd., with permission). |
Table 62.1 Anatomical Definitions of Lymph Node Stations | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 Figure 62.2 Right side border of lesser sac. The yellow line indicates peritoneal incision to further separate the greater omentum and the transverse colon mesentery (from Hoshi H. Standard D2 and modified nodal dissection for gastric adenocarcinoma. Surg Oncol Clin N Am. 2012;21(1):57–70). |
The Technique of the D2 Nodal Dissection (Common Portion for Both a Distal and a Total Gastrectomy) (Figs. 62.2 and 62.3)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


