FAST Examination for Trauma
Focused assessment with sonography for trauma (FAST) examination has largely replaced diagnostic peritoneal lavage for initial evaluation of the patient with multiple trauma. The examination is performed in the trauma room by trauma surgeons. An accurate knowledge of the ultrasound anatomy of the regions examined is crucial for accurate interpretation. The key finding on FAST is the presence of fluid in one of the four areas examined; that finding is indicative of some internal injury requiring further investigation or exploratory laparotomy. If FAST is negative at initial evaluation, repeat examination in 30 minutes may be warranted.
SCORE™, The Surgical Council on Resident Education, classified Focused assessment with sonography (FAST scan) as an “ESSENTIAL UNCOMMON” procedure.
STEPS IN PROCEDURE
3- to 5-MHz transducer
Patient supine, clamp Foley catheter
Subxiphoid Examination
Transducer placed in epigastric region, just under the xiphoid process
Firm downward pressure to allow sound wave to go under xiphoid process
Direct transducer cephalad and toward patient’s left shoulder
Right Upper Quadrant View
Transducer placed at midaxillary line just below right costal margin
Identify right kidney, then angle transducer upward to find liver
If difficulty is encountered, try a more posterior location
Left Upper Quadrant View
Transducer placed at midaxillary line just below costal margin
Angle transducer slightly downward to identify left kidney
Then slowly angle transducer upward to find spleen
Suprapubic View
Make sure that bladder is full
Place transducer in suprapubic region
Identify the two fossae on each side of bladder
HALLMARK ANATOMIC COMPLICATIONS
False-negative examination
Inability to access window because of overlying bowel gas
Inability to access window because of overlying bone or lung
LIST OF STRUCTURES
Xiphoid process
Pericardium
Liver
Right and left kidneys
Bladder
Paravesicular fossae
Transducer Placement Locations for Performing FAST (Fig. 43.1)
Technical Points
FAST is performed with a 3- to 5-MHz transducer placed sequentially in the following locations: Subxiphoid (to image the pericardium), right upper quadrant, left upper quadrant, suprapubic. In preparation for the examination, make sure that the patient has a full bladder by clamping the Foley catheter, if present. The purpose of the examination is simply to determine if fluid is, or is not, present in the locations examined. Fluid may be blood, gastric contents, bile, or succus. The examination is not designed to yield a definitive diagnosis. Interpretation of the FAST examination must be done in conjunction with clinical picture and other imaging studies. In some circumstances, a
repeat FAST examination may be helpful, because it takes time for blood or fluid to accumulate in these locations.
repeat FAST examination may be helpful, because it takes time for blood or fluid to accumulate in these locations.
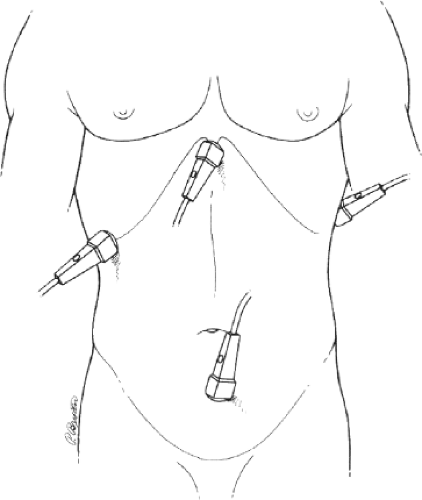 Figure 43.1 Transducer placement locations for performing focused abdominal sonography for trauma (from Rozycki GS, Ballard RB, Feliciano DV, et al. Surgeon-performed ultrasound for the assessment of truncal injuries. Lessons learned from 1,540 patients. Ann Surg. 228;4:557–567, with permission). |
Anatomic Points
These four locations are chosen for two reasons: First of all, they provide good ultrasound “windows” into the peritoneal cavity; second, they are regions were fluid accumulation is likely to occur in trauma.
The concept of an acoustic window is quite simple. Ultrasound is strongly reflected by interfaces between liquid/tissue and air (i.e., the lungs) or bone, and this reflection obscures the visualization of deeper structures. A good window avoids these interfaces. Thus the subxiphoid approach to the pericardium avoids potential overlap of ribs or lung and takes advantage of the anatomy illustrated in Chapter 20.
Free fluid most commonly results from bleeding from the spleen or liver. Initially this blood may accumulate under these organs, where it is detectable by examination of Morrison’s pouch or in the splenorenal space. Blood also tends to pool in the pelvis, where it may be picked up on suprapubic examination. Although it is true that blood will also be found around loops of small bowel or in the paracolic gutters, these regions are more difficult for the nonradiologist to interpret.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


