Fallopian Tube: Diagnosis
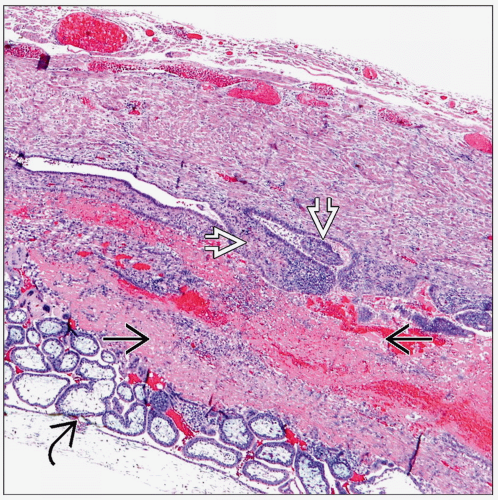 An ectopic pregnancy can be a medical emergency and is identified by immature placental villi  and implantation site and implantation site  within a fallopian tube. Fimbriae within a fallopian tube. Fimbriae  underlie the implantation site. underlie the implantation site. |
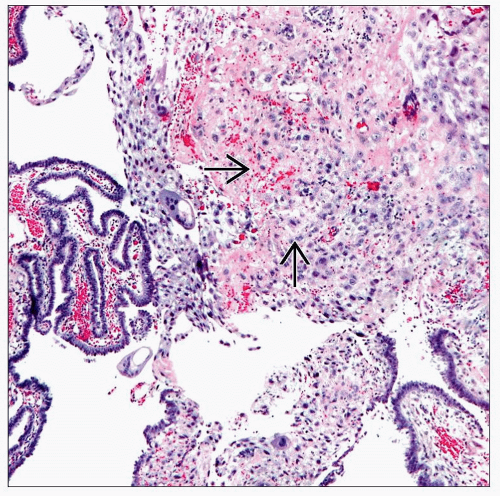 In the absence of villi and embryonic tissue, the presence of implantation site trophoblasts  in the wall of a fallopian tube is sufficient for the diagnosis of an ectopic gestation. in the wall of a fallopian tube is sufficient for the diagnosis of an ectopic gestation. |
SURGICAL/CLINICAL CONSIDERATIONS
Goal of Consultation
Determine if a mass-forming lesion of fallopian tube is benign or malignant
Diagnose suspected tubal pregnancies by identifying products of conception
Change in Patient Management
Additional biopsies may be taken for staging if carcinoma is present
If ectopic pregnancy is present, salpingectomy or salpingotomy is performed
Additional surgical exploration is not necessary to identify alternative sites
Clinical Setting
Majority of serous carcinomas are thought to arise in fimbriae of fallopian tubes
Women with BRCA1 or BRCA2 or P53 (Li-Fraumeni syndrome) germline mutations are at high risk
Tubal carcinoma is difficult to diagnose preoperatively
Inflammatory conditions are more common than malignancy
Women with elevated hCG levels but without documented intrauterine pregnancy may have ectopic pregnancy
Rupture and hemorrhage can be life threatening
Majority of cases are diagnosed by ultrasound and managed conservatively
In rare cases, clinical evaluation is inconclusive and intraoperative examination may be helpful
SPECIMEN EVALUATION
Gross
Describe size (length and diameter) and presence or absence of fimbriated end
Tubal carcinomas typically arise within fimbria
Close inspection for adhesions, discoloration, or masses is critical
Patency of lumen is determined with probe
Plastic ring may be present if there has been prior tubal ligation
Serosal surface is described
Normal: Smooth and glistening
Adhesions: Rough surface and attached tissue
Paratubal cysts
Purulent or fibrinous exudates
Rupture
For tubes removed as part of prophylactic salpingectomy
If grossly normal or if only cysts are present, fixation without sectioning is recommended
Likelihood of diagnosing carcinoma is very small
Detection of precursor lesions and small carcinomas may be compromised unless specimen is optimally fixed and processed
If a solid nodule > 0.5 cm is present and only a portion can be frozen, a frozen section may be appropriate
If a mass is present in tube
Make serial cross sections of tube; note any tubal contents
Purulent exudate
Hemorrhage
Placental or fetal tissue with membranes
Masses
Areas of firmness or discoloration
Frozen Section
If solid mass is present, a portion may be frozen to determine if carcinoma is present
In setting of suspected ectopic pregnancies, areas of hemorrhage and blood clot often contain products of conception if they are not readily evident
MOST COMMON DIAGNOSES
Serous Lesions
Serous tubal intraepithelial carcinoma (STIC)
May be seen in areas adjacent to invasive carcinoma
Identified at low power by irregular epithelial thickness with exfoliation of tumor cells
High nuclear to cytoplasmic ratio and loss of cilia
Nuclei show marked pleomorphism
Enlarged nuclei with prominent nucleoli
Frequent mitoses
Hyperchromasia
Apoptotic bodies common
May require supportive immunohistochemical studies for p53 and Ki-67 for diagnosis
Invasive serous carcinoma
90% of fallopian tube carcinomas
3-20% are bilateral
Similar histologic features as mentioned above with invasion into underlying stroma
Frequently associated with lymphovascular invasion, which may be identified on frozen sections
Ectopic Pregnancy
Most common implantation site for ectopic pregnancy is fallopian tube
87-99% of tubal pregnancies can be diagnosed by transvaginal ultrasound
Only rare women have a positive pregnancy test and inconclusive ultrasound examinations
Surgical treatment can be by salpingotomy or salpingectomy
Intraoperative evaluation may be useful for cases with unclear clinical and imaging characteristics
Presence of fetal villi, gestational sac, implantation site, or embryonic parts is diagnostic
Infarction
Edematous, hemorrhagic tube grossly
Widespread hemorrhagic necrosis commonly present microscopically
Transitional Cell Lesions
Transitional cell metaplasia
Also termed Walthard nests
Common benign finding; not proven to be a precursor lesion
Transitional cell carcinoma
10% of primary fallopian tube carcinomas
Histologic appearance is similar to urinary tract transitional carcinomas
Solid and papillary sheet-like growth
High-grade nuclei
Frequent mitoses
Inflammatory Conditions
Can be associated with endometriosis, pelvic inflammatory disease, and chronic endometritis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


