|
 Figure 2.1.1 Florid hyperplasia without atypia: A terminal duct lobular unit is expanded by proliferating epithelial cells; the proliferation is confined to the lobular unit without involving an adjacent true duct. |
 Figure 2.1.6 ADH: Several lobular units have dilated acini that show epithelial hyperplasia. |
 Figure 2.1.2 The secondary spaces created by the epithelial hyperplasia have an irregular shape. |
 Figure 2.1.3 Secondary spaces are fenestrated and not sharply defined in florid hyperplasia without atypia. |
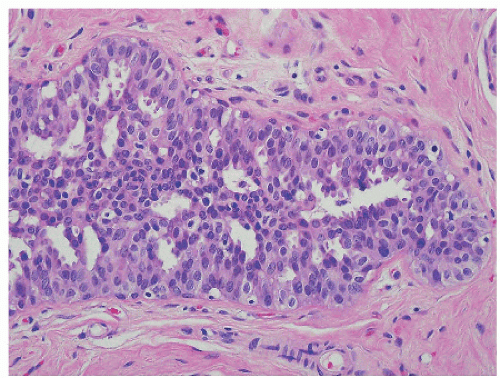 Figure 2.1.4 The irregular secondary spaces are a manifestation of uneven cell placement; note nuclear variability and overlap in this example of florid hyperplasia without atypia. |
 Figure 2.1.7 The two acini in the center contain a proliferation of epithelial cells; secondary spaces are peripheral but uniform in this example of ADH. Microcalcifications are present in one of the involved acini. |
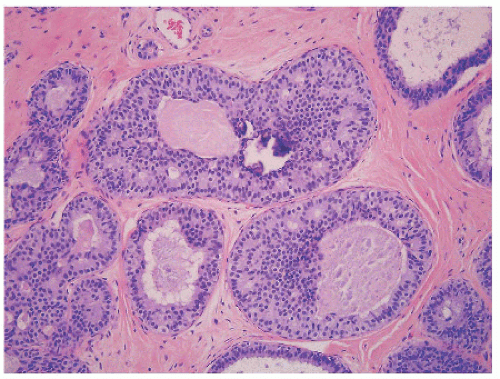 Figure 2.1.8 Nuclear uniformity and even cell placement characterize ADH. |
 Figure 2.1.9 The uniform cells of ADH form small microrosettes. Cell borders are evident. |
 Figure 2.1.5 Fewer secondary spaces are present in this solid, compact focus of florid hyperplasia without atypia, recognized by nuclear variability and overlap. |
|
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


