Gastrointestinal (GI) infections are a major cause of morbidity and mortality on a global scale, second only to upper respiratory tract infections. The global mortality rates were estimated to be 5 to 10 million per year around 1980, which decreased to about 3 million in 1992 and further to 1.5 million by 2005.1, 2 Of these, it is estimated that about 70% cases are foodborne.3 The global mortality in children aged less that 5 has also decreased from 13.6/1,000 to about 5/1,000 during this time, largely due to implementation of oral rehydration and improved supportive therapy. In the United States, it has been estimated that about 76 million foodborne illnesses occur annually that result in 3,250,000 hospitalizations and 5,200 deaths.4 Although the mortality from GI infections has decreased worldwide over the years, its incidence has remained the same and it still remains one of the major health concerns, being second in frequency only to the common cold. Our understanding of the causes of infectious diarrhea was also limited prior to 1970, with the exception of sporadic outbreaks of Salmonella, Shigella, or enteropathogenic Escherichia coli, which were the major recognized pathogens. With time, the number of infectious organisms recognized to cause GI infections has greatly increased, as has our understanding of their pathogenesis and host defense mechanisms.5 Common causes of GI infections according to classes of organisms and their main clinical presentation and diagnostic methods are shown in Table 19-1.
HOST DEFENSE MECHANISMS
Enteric infections result when the host defense mechanisms are overwhelmed by the infection or are intrinsically defective. Thus, a brief review of the normal host defense mechanisms is helpful in understanding the pathogenesis of many enteric infections. Immune and nonimmune mechanisms play an important role in host defenses. For a more detailed discussion of host immune system, see Chapters 3 and 4.
Acidity of Gastric Juices
The normal low pH of gastric juice is lethal for most organisms ingested with food and drink. Patients with hypochlorhydria or achlorhydria due to atrophic gastritis, postgastrectomy states, or gastroenterostomy, and even smoking cannabis,6 have an increased frequency of GI infections, particularly by bacteria such as Shigella and Salmonella.7, 8 However, ingested food buffers gastric pH and a time lag before gastric pH is maximally reduced may allow some organisms to pass through the pylorus before getting killed. Therapeutic acid suppression with proton pump inhibitors (PPIs) has also been suggested to increase the incidence of GI infections, although it remains somewhat controversial.9, 10 It is clear that many organisms can survive the gastric transit and establish themselves in the intestines.
Intestinal Motility
Normal peristaltic activity prevents bacterial accumulation. When there is stagnation of intestinal contents, as in the blind-loop syndrome, intestinal pseudo-obstruction, and possibly surgically constructed intestinal pouches and reservoirs, bacterial overgrowth occurs, with resultant diarrhea or steatorrhea.11
Table 19-1 Important Enteric Infections Classified According to Major Classes or Organisms
INFECTIOUS AGENT
RISK GROUP/EPIDEMIOLOGY
CLINICAL MANIFESTATIONS
DIAGNOSIS (SPECIAL TECHNIQUES ARE RARELY USED IN SELF-LIMITED INFECTIONS)
Bacteria
Staphylococcus aureus
Gram-positive cocci
Food poisoning, clustered in small groups, family members, restaurants, nursing homes
Profuse watery diarrhea, nausea, vomiting, abdominal cramps within 12 h of food ingestion
Toxin assays, primarily for research or public health use
Escherichia coli
Gram-negative bacillus
Enterotoxigenic
Traveler’s diarrhea
Food and water borne
Diarrhea, cholera-like but less voluminous; abdominal cramps
The mucin covering the surface not only provides a physical barrier, but also allows adherence by many commensal bacteria that competitively inhibit binding of the pathogenetic organisms. The secretion of mucins can be modified by activation of pathogen recognition receptors and toll-like receptors present on the epithelial cells.12 The goblet cells secrete a mucin (Muc2) that has a protective effect against luminal infectious organisms.12, 13, 14 Intestinal mucus also contains secretions of Paneth cells that include lysozyme, alpha-defensins, secretory phopholipase-2, cryptdin-related sequence peptides, and angiogenin-4 (see Chapter 16). Paneth cells secrete these antibacterial products at high levels in response to cholinergic stimuli and when exposed to bacterial antigens.15, 16 These antibacterial products act in conjunction with intestinal peristalsis to expel bacteria from the gut lumen. It may also have a lytic action on bacteria.1 Mice transgenic for a human Paneth cell alpha-defensin, HD-5, are completely immune to infection and systemic disease from orally administered Salmonella enterica serovar typhimurium.17 Interestingly, it has also been shown that newborn mice that are susceptible to infection by Shigella become resistant to the infection by day 7 when the Paneth cells develop.18 In humans, lack of Paneth cells in newborn infants has been linked to development of neonatal necrotizing enterocolitis.19 It is believed that lack of lysozyme may render these infants susceptible to bacterial translocation and subsequent sepsis. On the other hand, Paneth cell metaplasia in the colon in various chronic inflammatory conditions including inflammatory bowel disease (IBD) may be an attempt to protect the damaged epithelium from luminal microbes.
Normal Resident Bacterial Flora
Each segment of the GI tract from the mouth down to the anus may be colonized by its own specific microflora, which usually live in symbiosis with the host and prevent proliferation of potential pathogens. A good example of the harmful effect of the change in the internal bacterial milieu is seen in patients following antibiotic therapy who develop pseudomembranous colitis. In these patients, the normal resident bacterial flora is eliminated or markedly altered, allowing proliferation of organisms such as Clostridium difficile, a pathogenic organism that causes mucosal damage by the production of an enterotoxin, often with resulting pseudomembranous colitis. There is also an association between diarrheal disease in humans and antibiotics in animal feed. The large-scale feeding of broad-spectrum antibiotics to farm animals, used to promote growth, has led to their colonization by antibiotic-resistant bacteria.2, 20 Alterations in the gut flora have also been implicated in motility disorders like postinfectious diarrhea and irritable bowel syndrome.21, 22
Gut-Associated Immune System
One of the major functions of the gut immune system is to prevent bacterial, viral, and parasitic infections.23, 24 This protection is provided within the lumen by secretory IgA and within the mucosa by inflammatory cells, including plasma cells, eosinophils, lymphocytes, and macrophages. Secretory IgA lines the bowel mucosa, and is very efficient at agglutinating bacteria and viruses and neutralizing toxins. Those antigens that escape the action of secretory IgA and penetrate the surface epithelium, or are deliberately transported across M cells (see Chapter 16), are dealt with by locally sensitized lymphocytes that include lamina propria B, T, and NK cells,25 by combination with preformed antibodies or by ingestion by macrophages. As might be anticipated, patients with primary, acquired, or iatrogenic immunodeficiency disorders are particularly prone to GI infections, especially with unusual organisms such as Mycobacterium avium-intracellulare and Cryptosporidium. These infections also tend to be more severe, prolonged, and resistant to therapy than those in immunocompetent individuals.
The type of infection found in immunocompromised patients depends on the specific immunologic defect. Thus, patients with impaired B-cell function are most prone to bacterial infections and protozoa such as Giardia, while those with impaired T-cell function and defective cell-mediated immunity have a susceptibility to a variety of viral, fungal, and mycobacterial infections.26 For example, patients with acquired immunodeficiency syndrome (AIDS) are prone to infections with Candida, cytomegalovirus (CMV), herpes, Cryptosporidium, and M. avium-intracellulare among many others (see Chapter 3). Superinfection with strongyloidiasis is found in patients on steroids or those who have undergone granulocytetargeted chemotherapy or organ transplantation.
Infection of the Normal Host
Although abnormalities of the host defense mechanisms predispose to enteric infections as enumerated above, it must be stressed that the majority of patients with GI infections have no known defect. In most patients, the gut defenses are evaded, deceived, or simply overwhelmed by infection with massive numbers of proliferating organisms or enterotoxins.
MECHANISMS OF INFECTION
For organisms such as bacteria to cause symptoms, they have to either invade the mucosa or produce an exotoxin that acts directly on the epithelium, as seen, for instance, with some Clostridia or with ingestion of preformed toxins. More usually, the organism has to approach, attach to, and colonize epithelial cells. This process of colonization and continued toxin production is necessary for many organisms, such as amoebae, Vibrio, E. coli, Yersinia, Shigella, Salmonella, Giardia, and many other relatively common pathogens including worms such as Strongyloides. The series of events leading up to attachment and colonization is therefore critical in many enteric infections in which the mechanism of disease production is understood.
Adherence, Initial Attachment, and Colonization
Binding of organisms to the cell surface is probably a multistage process. Initially there is passage through the mucous layer, allowing contact with epithelial cells and weak attachment to them. However, some organisms, such as Vibrio, may have greater adherence to the mucous layer than to the underlying epithelial cells.27 Attachment of organisms to epithelium is initially very fragile and easily disrupted experimentally by simple washing, for instance. Nevertheless, this likely does not represent nonspecific adhesion but rather the presence of both specific epithelial receptors, which are probably oligosaccharides, and the ability of the organism to produce appropriate fimbrial proteins recognizing these receptor sites. Next, there is a tighter attachment resulting from the formation of fimbrial “adhesions.” Colonization results from multiplication of successful organisms. Following colonization, several different mechanisms have been described that result in the production of symptoms. These have been best classified in diseases caused by E. coli, which were initially described as being enteropathogenic. Following this, several related but distinctive mechanisms were delineated for other E. coli organisms, which included enteroinvasive (EIEC), enterotoxigenic (ETEC), enterohemorrhagic (EHEC), and enteroadherent E. coli (EAEC).28 These have in common that, with the possible exception of enteroadherent organisms, after colonization of the epithelium they probably all produce toxins, while the enteroinvasive organisms have the additional property of invasion. While these jingoistic terms have been utilized primarily for E. coli, they can be expanded as a template to describe the mechanism of action of virtually all of the enteric organisms causing acute diarrhea.
Tissue Invasion
Enteroinvasive organisms attach to and invade epithelium. The result is some degree of necrosis and an acute inflammatory infiltrate, followed by local and systemic immune response and repair. Surface ulceration results in the shedding of neutrophils and red cells into the lumen, where they can be detected in the stools together with epithelial cells. Included in this group mechanistically are numerous well-recognized bacteria, including Shigella, Salmonella, some E. coli serotypes, Campylobacter jejuni, Campylobacter coli and Yersinia, protozoa including Amoebae, and worms such as Strongyloides. The degree of damage depends on numerous factors, including virulence, motility, toxin production, ability of cells to induce their endocytosis, ability to replicate within cells, and host immunity. Shigella, some E. coli serotypes, and Campylobacter multiply within epithelial cells and are deposited either in the basolateral space or in the cytoplasm, where they continue to replicate and ultimately kill the epithelial cell. Some organisms, such as S. typhi and S. paratyphi may be transmitted into the lamina propria, with relatively limited epithelial damage. Others like Salmonella and Yersinia organisms tend to cause necrosis primarily in the M-cell regions overlying lymphoid aggregates. The ensuing enteritis or colitis can extend to involve regional lymph nodes, and with some organisms such as Salmonella, the infection may become systemic.
Because most of these organisms, specifically Shigella and some E. coli organisms, produce Shiga or a Shiga-like toxin mediated by a 140-kD plasmid, injury can be expected in cells not necessarily containing the bacteria. Electron microscopic examination shows degenerative changes in the epithelial and endothelial cells in the apparent absence of bacteria, and therefore implying possibly toxin-related injury; capillary endothelial damage is invariably present and may potentiate the mucosal injury. However, while some bacteria-containing cells are clearly damaged, others show virtually no changes.29 It is unclear whether unaffected cells remain so, or whether all of them ultimately die.
Toxin Production
Toxin production appears to be essential to many infections. These organisms can cause diarrhea either by producing powerful exotoxins without necessarily attaching to, invading, or destroying epithelial cells or by toxin production following colonization of the epithelium, although any or all of these combinations may occur.
C. difficile produces its effects by virtue of both exotoxins and cytotoxins, which do not require attachment or invasion but can be cytotoxic. This results in a spectrum of morphologic changes ranging from minimal inflammation to typical acute infectious (self-limited) colitis to pseudomembranous colitis. Other clostridial toxins (C. botulinum, C. perfringens) are preformed and ingested.
These are preformed toxins causing symptoms following ingestion. Six Staphylococcus enterotoxins have been identified (A-F) and all have been associated with GI symptoms following ingestion, although precisely how this is achieved is unclear. This is a common toxin in pre-prepared and reheated foods. Although symptoms may be severe, they are usually short-lived.
Perhaps the prototype of the enterotoxigenic organisms is the plasmid-mediated cholera toxin produced by vibrios causing epidemic watery diarrhea, particularly in parts of Asia. An identical plasmid carried by some E. coli serotypes and possibly Plesiomonas causes these organisms to produce the same toxin, massive watery diarrhea with a high mortality in children, and some forms of traveler’s diarrhea in adults. For the toxin to be effective, the organism must be attached to epithelium, but it is not invasive or destructive. The toxin can be blocked with oral vaccines and offer considerable protection.
Many bacteria produce Shiga toxins; these are particularly enigmatic in that the two major toxins produced are the serotype 1-like toxin and verotoxin. The serotype 1-like toxin is produced classically by Shigella dysenteriae, but is also elicited by numerous other organisms, including other Shigella serotypes, some E. coli serotypes, and vibrios, and requires colonization of the epithelium. The problem is that while numerous bacteria have the ability to produce Shiga toxin, they can produce it in high, low, or intermediate quantities, which do not readily correlate with symptoms.
Virtually all of the GI pathogenic bacteria elicit Shiga toxin, although the precise role that it plays is currently unclear. Shiga toxin causes permanent adenyl cyclase activity resulting in persistent secretion. Verotoxin production is important because of its clinicopathologic associations. The first of these is diarrhea occurring in all age groups and is the result of ingesting the organism, usually the E. coli O157:H7 serotype (VTEC) but occasionally Shigella, Salmonella, and Campylobacter, particularly in food that is pre-prepared, such as in institutions, or from undercooked food from fast food outlets, particularly hamburgers or, less frequently, unpasteurized milk. Verotoxin was identified because of its effect on vera monkey kidney cells in culture and was first isolated from E. coli 026.30 Interestingly, removal of the plasmids seemed not to affect toxin production. The toxin appears to be unlike cholera toxin in that it seems to have no effect on adenylate cyclase activity. Verotoxin has been found to be produced by E. coli serotypes, especially serotype O157, and occasionally by other organisms such as Campylobacter, Shigella, and Salmonella.
Verotoxin production characterizes the enterohemorrhagic group of diseases. Verotoxin production is also associated with the hemolytic uremic syndrome (HUS) and thrombotic thrombocytopenic purpura (TTP) in children, and in the elderly with hemorrhagic enterocolitis, which has an appreciable mortality. Verotoxin likely causes endothelial damage, which can result in leak of plasma and red cells (hence diarrhea and hemorrhage), with subsequent absorption and endotoxemia causing thrombosis both locally and at distal sites, but particularly in the kidney (hence the HUS), with platelet sequestration (hence purpura) resulting from or associated with impaired aggregability and depletion of serotonin, adenosine diphosphate (ADP), and β-thromboglublin.31
Enteroadherent and Other Mechanisms of Diarrhea
Some E. coli are able to cause diarrhea without being toxigenic and invasive. Some of these have the ability to attach to epithelial cells due to production of a 94-kD protein known as EPEC attachment factor. Some of the type II enteropathogenic E. coli seem to have this property and are definable by their diffuse attachment to HEp-2 cells. A variety of other organisms are also likely to be mechanistically similar, and attach to the luminal border of cells throughout the GI tract. These include H. pylori in the stomach, Giardia and Cryptosporidium in the small intestine, and nontreponemal spirochetes causing intestinal spirochetosis in the large intestine.
Persistence of Infection
Some organisms persist either attached to the apical portion of cells or within the bowel wall. This is potentiated by immunodeficiency states including AIDS when organisms such as Cryptosporidium or Mycobacterium avium-intracellulare may become chronic. Even in apparently immunologically competent individuals, infections such as those caused by Whipple’s disease, Salmonella, and Mycobacterium may cause chronic disease, while others, such as Brachyspira (causing intestinal spirochetosis), may remain attached to epithelium without clearly producing disease.
APPROACH TO DIAGNOSIS OF GI INFECTIONS
Introduction
The majority of GI infections, particularly gastroenteritis with diarrhea, are diagnosed on clinical grounds without the help of stool examination, microbiology cultures, or serologies; indeed a large proportion are E. coli and are not captured on routine culture. On most occasions, even the diagnosis of a specific infection is not necessary or (depending on the resources available) cannot be pursued, and one either waits for the resolution of symptoms or starts empiric therapy, more so if a specific infection is known to be endemic in that area. This is the case with viral diarrheal syndromes, or amebiasis in endemic areas. Thus pathologists rarely see biopsies from such conditions, and even the spectrum of pathologic changes in many of these infections remains poorly studied and described in the literature. However, in some cases an infection comes to attention for the first time based on a biopsy. Many esophageal and gastric infections are diagnosed for the first time with biopsies, while biopsies are reserved for special situations in intestinal and colonic infections. On such occasions, the biopsy may provide a specific diagnosis (e.g., CMV infection), or identify a broad group of organisms (e.g., yeast forms in tissues or identification of acid-fast organisms) where identification of specific organism may require cultures or other studies, or may identify a tissue reaction associated with a limited number of organisms thus narrowing the differential diagnosis (e.g., granulomatous inflammation or suppurative inflammation) (Table 19-2). Biopsy in many situations provides a rapid diagnosis of the underlying infection, while other studies may take longer, much longer in some mycobacterial and fungal infections, and is critical in initiating early treatment, for example, CMV infection in a post-bone marrow transplant (BMT) or stem cell transplant (SCT) patient. However, it is imperative that the pathologist is provided with the pertinent clinically important information and judiciously use additional studies to confirm or support the diagnosis (special stains, immunohistochemistry [IHC] or molecular tests). It is essential that the pathologists clearly understand the clinical situation, what is asked of them, and the resources available to fulfill their role. This requires integration of clinical findings, gross and endoscopic findings, other laboratory data, pathologic findings, and appropriate triaging of tissues for ancillary tests. The subsequent discussion is a brief outline of such an approach.
Table 19-2 Pathogens Causing Distinctive Cellular Changes or Tissue Reactions
Cytopathic or Cytoproliferative Reaction
Granulomatous Reaction (Necrotizing)
Adenoviruses
Nontuberculous mycobacteria
Measles virus
Bartonella henselae
Cytomegalovirus
Chlamydia trachomatis
Varicella-zoster virus
Yersinia enterocolitica
Herpes simplex viruses 1 and 2
Yersinia pseudotuberculosis
Human papillomaviruses
Necrotizing Reaction with Little Inflammation
Cytoplasmic Granularity
Clostridium
Cystoisospora
Enterohemorrhagic Escherichia coli
Microsporidia (Enterocytozoon intestinalis)
Zygomycosis
Toxoplasma gondii
Foam Cell Reaction
Tropheryma whippleii
Mycobacterium avium complex
Histoplasma capsulatum
Rhodococcus equi
Granulomatous Reaction (Noncaseating)
Mycobacteria
Histoplasma capsulatum
Brucella
Schistosoma
Toxoplasma gondii
Whipple’s disease
Granulomatous Reaction (Caseating)
Mycobacteria
Histoplasma capsulatum
Aspergillus
Cryptococcus neoformans
Brucella
Nocardia
Clinical Features
Understanding the clinical setting and the clinical differential diagnosis is often of paramount importance for proper interpretation of the pathologic findings. It cannot be overemphasized that the knowledge of the immune status of the patient and the degree and nature of any immunodeficiency present is very important. While immunodeficiencies predispose patients to opportunistic infections, the frequency of these infections varies depending on the nature of the immunodeficiency; a different (though overlapping) set of opportunistic infections occur in T-cell-deficient versus neutropenic patients.
The clinical features depend on the organisms and their mechanisms of actions, such as toxin production or direct injury by a cytotoxic effect. Some of the organisms produce a secretory-type diarrhea, which usually is nonbloody and watery, and in which an exudate of neutrophils is not prominent, while others produce dysenteric symptoms characterized by diarrhea, which is often bloody, abdominal cramps, fever, and leukocytes or elevated lactoferrin in the stool. Systemic manifestations such as rigor, fever, and headaches presumably result from inflammation or bacterial invasion of the mucosa, from bacteremia, or from toxin activity.
In general, infectious gastroenteritis are typically broken into inflammatory, secretory, and malabsorptive categories, and into acute, subacute, or chronic durations, and may produce a spectrum of clinical findings ranging from minimal symptoms to a disease resembling ulcerative colitis clinically and endoscopically. These conditions can simplistically be classified as (gastro) enteritic, colitic, proctitic, or anal/perianal; combinations of them may occur in anatomically adjoining parts of the bowel.
Enteritis refers to a malabsorption-type diarrhea, often with little abdominal pain or fever but voluminous stool; the symptoms of colitis are generally a smaller volume of diarrhea, which may be bloody, prominent abdominal cramping, and commonly fever. Gastroenteritis frequently refers to a syndrome in which diarrhea, nausea, and vomiting are represented to varying degrees. Proctitis is characterized by normally formed stool but with rectal urgency, perianal discomfort, rectal bleeding, and passage of mucus (and sometimes constipation instead of diarrhea); anal/perianal symptoms are primarily those of local pain, pruritus, or both. Diarrhea when present can be classified as either acute or chronic, and as nonbloody or bloody. Other clinical scenarios include vomiting without diarrhea, diarrhea in the immunocompromised host, anorectal symptoms without diarrhea, and traveler’s diarrhea. These are discussed subsequently in the later sections.
Endoscopic and Gross Findings
It is important that clinicians and pathologists recognize the gross/endoscopic appearance of various infections as this provides an opportunity early enough in the workup of a patient for obtaining appropriate samples for workup of infections: for example, viral culture, stool culture, serology, and so on. The endoscopic and gross findings can range from normal or minimal changes, to marked mucosal abnormalities mimicking IBD. Some of the pathogens like Vibrio or Cryptosporidium typically produce no or minimal gross changes in the mucosa, while some tend to produce typically ulcerative disease (CMV, Herpes, amebiasis). The nature of ulcers with CMV, Herpes, and amebiasis are often distinctive and knowledge of the typical endoscopic changes associated with various infections often gives a clue to the underlying infection. Focal ulcers may be seen in amebic infection, while aphthoid ulcers can be seen in Yersinia and sometimes Chlamydia infections. Presence of pseudomembranes makes the possibility of C. difficile infection most likely, although it may sometimes be seen with ischemia or other toxin-producing organisms like Salmonella, Shigella, or EHEC. Enteroinvasive organisms produce an appearance that may range from normal, mucosal edema, mild and patchy erythema, or be indistinguishable from ulcerative colitis or proctitis. Verotoxin-producing organisms may cause a hemorrhagic colitis that may also be primarily right-sided, while in immunosuppressed patients neutropenic enterocolitis primarily tends to involve the cecum and right colon. Mycobacterium avium-intracellulare complex (MAI or MAC) tends to produce plaque-like or nodular lesions, while the presence of ileocecal strictures should make one suspect tuberculosis in endemic areas, as well as Crohn’s disease. On many occasions, the changes are simply of a nonspecific colitis. The range of mucosal abnormalities associated with some infections is also wide; CMV infection may be associated with normal-appearing mucosa or with extensive ulcerations and inflammation mimicking IBD. C. difficile also produces changes ranging from redness to pseudomembranous colitis that may be most marked proximally or extend to the rectum.
Stool Examination, Culture, and Other Studies
A variety of tests that include stool microscopy for ova and parasites, culture, stool antigen assays, and serology are available to aid in the diagnosis of GI infections. The differential diagnosis of enteric infection varies with age, socioeconomic status, risk behaviors, geographic location, and other clinical and epidemiologic variables. Enteric infections found in North America are different from those of less-developed countries. In addition, the type of infection an individual is susceptible to varies according to environmental and host factors. For example, the likely offending organisms in patients with traveler’s diarrhea are different from those in patients with food-associated infection or from those in persons following oral-anal sexual practices or who are immunocompromised. Based on the clinical scenario, clinicians should be aware of the differential diagnosis and choose the best tests. Providers must also be aware of the available resources, prevalent practices in their microbiology lab, and the meaning of the results of various laboratory tests.
Stool cultures are often requested in patients with diarrhea; however, it is important to recognize the limitations of the techniques. Most labs plate stools to selective agar both directly and after selective broth enrichment. Selective media for Salmonella, Shigella, and Campylobacter are routinely employed. Many labs require separate request to test for Yersinia enterocolitica. Testing for E. coli O157:H7 or other Shiga toxin-producing organisms using a combination of culture and Shiga toxin enzyme immunoassay is recommended by current guidelines but may not be routinely performed, as the testing is expensive and the diseases uncommon. Without specific requests most labs in United States will typically not specifically test for Vibrio species, Aeromonas, and Plesiomonas. Stool culture for detection of C. difficile is time-consuming and nonspecific, as culture does not differentiate pathogenic and nonpathogenic strains. Hence, nonculture diagnostic strategies have been developed and are widely used. These include detection of the toxin by cytotoxicity, by antigen detection, or by polymerase chain reaction (PCR) for the toxin gene. For mycobacteria special culture media need to be used, so specific studies must be ordered. Molecular studies for detection of mycobacteria and other bacteria are available from specialized reference labs. In patients with anorectal symptoms (tenesmus, perianal pruritus, blood, or pus) without overt diarrhea a possibility of a sexually transmitted disease should be considered, especially if there is a history of anoreceptive intercourse. Workup should include evaluation for Chlamydia, Neisseria gonorrhoeae, syphilis and herpes simplex virus (HSV) infection. Workup of suspected viral diarrhea may include commercially available antigen-based diagnostic tests that will rapidly detect rotavirus. PCR-based assays for caliciviruses (including norovirus) are becoming more widely available, though none are FDA approved; tests for detection of astrovirus and other GI viruses are available primarily on a research basis. Methods for identification of various parasites use examination of wet mount specimen of stool with or without special stains and involve identification of ova or the pathogen. Antigen detection is the test of choice for Cryptosporidium and Giardia, and for Entamoeba histolytica as well, though the latter test is less widely available. PCR-based assays have been developed for many of the pathogens but are not widely available. The range of infections in various immunocompromised settings is discussed later.
In the setting of acute nonbloody diarrhea, the likelihood of recovering a pathogen from stool cultures is low, especially if the patient lacks significant abdominal pain, tenderness, fever, recent travel history, and multiple stools in the 24 hours preceding the presentation.32, 33 With chronic diarrhea, the workup should include evaluation for C. difficile in patients exposed to antibiotics, as well as Giardia and Cryptosporidium. Acute bloody diarrhea, on the other hand, is often a medical and possibly a public health emergency and cultures should always be obtained for a variety of pathogens that include Campylobacter, Shiga toxin-producing E. coli, including the O157:H7 strain and others, Salmonella and Shigella. C. difficile should also be included, although community-acquired C. difficile is less common and may develop more gradually than other bacterial infections causing bloody diarrhea. Workup should also be considered for chronic bloody diarrhea (e.g., lasting more than 2 weeks) as IBD becomes an important consideration, and infections still need to be excluded. Workup should include evaluation for the list of organisms above associated with acute bloody diarrhea, as well as parasites including Entamoeba histolytica or Balantidium coli, especially if there is a history of travel to an endemic area. Vomiting without diarrhea or minimal diarrhea is most often suggestive of a viral infection, most likely a norovirus, or a preformed bacterial toxin, like staphylococcal enterotoxin. It is often difficult to find an etiologic agent; however, most of these illnesses resolve spontaneously and rapidly. Testing for norovirus can be considered in sporadic as well as outbreak and health care-associated cases.
The clinician needs to be aware of these diagnostic tests and should work in close association with the pathologist, endoscopist, and microbiologist to ensure that the appropriate collection and laboratory techniques have been utilized in order to maximize the diagnostic yield. The decision to pursue a definitive pathogen depends on the clinical scenario, available resources, epidemiologic considerations, and the likelihood that the results will benefit patients, alter therapy, or have public health significance.
Biopsy Diagnosis
Most enteric infections are self-limited and, with an appropriate history, usually require no further investigation or, at most, stool culture and examination for ova and parasites. Endoscopic biopsy is reserved for those patients in whom it is important to exclude other causes of enteric inflammation, such as IBD and ischemia, or in whom it is essential to determine the specific infective agent in an attempt to alleviate debilitating symptoms. Sometimes, a negative histologic finding can be important, as it might indicate another site of infection, such as the small bowel instead of the colon, or a noninfectious cause of the patient’s symptoms.
Although the list of organisms causing enteric infections is very large, many produce the similar spectra of histologic changes, and attention to the histologic pattern can provide a clue to the diagnosis or a good differential diagnosis (Table 19-2). In immunocompromised patients such as those with HIV/AIDS, chemotherapy, or posttransplantation patients, a wider spectrum of infections may occur, with atypical mucosal reactions.26
The histologic changes fall into five major categories; each will be discussed in more detail.
No change. Cholera is the classic example. The causative organism Vibrio cholerae becomes adherent to the small intestinal villus, secreting an enterotoxin that induces a voluminous, potentially life-threatening secretory diarrhea, but does not injure the mucosa, although vacuolation of epithelium may occur. Many of the pathogens occasionally produce virtually no histologic abnormality, mostly viruses. Also, some organisms can exist in a carrier state in which they are not pathogenic to the patient, do not produce symptoms, and are associated with a normal mucosa.
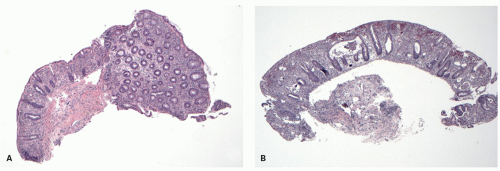
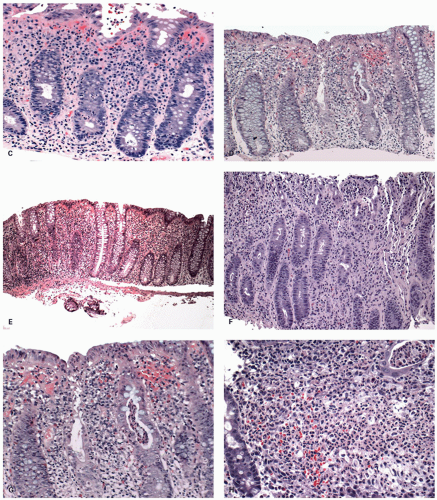
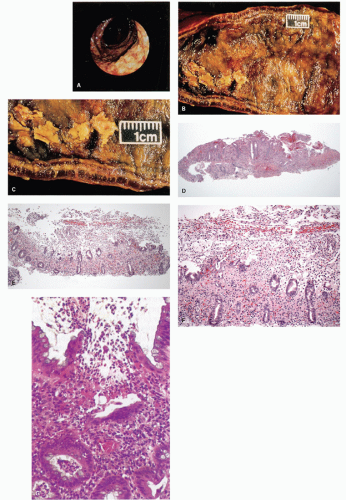
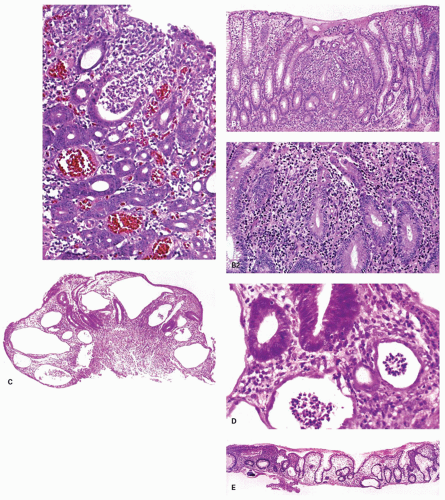
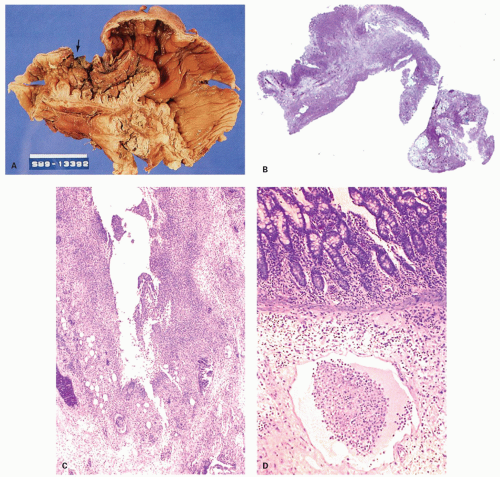
Figure 19-1. Acute infectious (self-limited colitis). Irrespective of whether an organism is isolated or not, this histologic appearance invariably resolves spontaneously. A: Overview of a biopsy showing a half of the biopsy fragment that is well oriented and reveals normal architecture with regularly spaced crypts that are largely parallel, but may be slightly pushed apart by edema and inflammatory infiltrate. The inflammatory infiltrate may be primarily limited to the upper two-thirds of the mucosa but, as shown here, it may extend down to the muscularis mucosae. The orientation of the crypts is difficult to assess in poorly oriented biopsies as seen here where half of the fragment is tangentially sectioned. Even in the poorly oriented part one can note that at least the crypts are evenly spaced and the lamina propria is expanded. B: There may be some degree of crypt distortion and crypt loss depending on the nature and severity of the infection as seen here. The density and proportion of inflammatory cell component in the lamina propria varies from being mild (C, D) to marked (E, F). Also note that there is often marked mucin depletion of the crypts and variable amount of neutrophilic infiltration of the crypts (cryptitis).
Typical acute infectious (self-limited) colitis. This is the most common change seen in enteric infections in the hospital setting. It is characterized histologically by lack of both the architectural distortion and basal lymphoid or plasmacytic infiltrate that characterize IBD, and by the presence of mucosal hyperemia, edema, and if severe by acute inflammation, with neutrophilic infiltration of crypts (cryptitis and crypt abscesses) (Fig. 19-1).34, 35, 36, 37, 38, 39 Crypt abscesses tend to occur in the mid and upper crypt, and may all be at an identical level in the mucosa. Sometimes the lamina propria contains a sea of neutrophils that is also characteristic of a severe infection. Crypts may be attenuated superficially, a finding also associated with pseudomembranous colitis, while the bases of the crypts may be pointed. Later during regeneration one may see focal cryptitis, some crypt branching, or distortion in those infections severe enough to cause crypt destruction, abscesses, or ulcers. Biopsy diagnosis of acute infection is usually possible only within the first days or sometimes few weeks of infection.
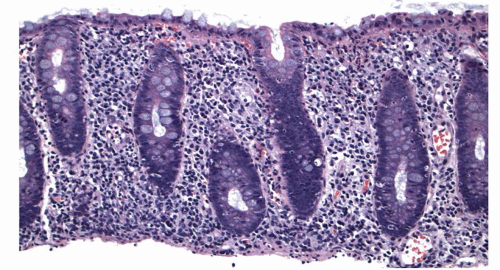
Figure 19-1.(Continued)G: The cryptitis tends to involve either the top part of the crypt or its entire length as opposed to crypt bases as seen with IBD. Neutrophils can also be seen in the lumen (crypt abscess) of the crypts frequently. H: In some patients the neutrophils in capillaries and lamina propria can be so intense as to be purulent.
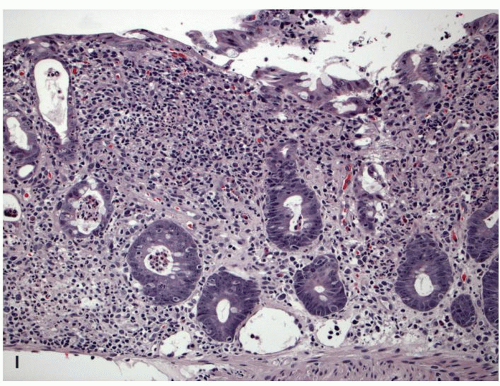
Figure 19-1.(Continued)I: Also note that in most cases although neutrophils are present in the lamina propria, the predominant inflammatory cells may still be plasma cells and lymphocytes. If an excess of inflammatory cells is present above the muscularis mucosae, there are very few plasma cells in this zone, the infiltrate being lymphohistiocytic and containing eosinophils and often neutrophils. The dense band of lymphocytes or plasma cells above the muscularis mucosae as seen in IBD is also not present.
Abnormal crypt architecture and chronic inflammation are closely associated with IBD, but can also occur in some severe enteric infections such as pseudomembranous colitis, shigellosis, Campylobacter, Chlamydia trachomatosis, syphilis, and herpesvirus.40, 41, 42 Conversely, patients without architectural distortion may ultimately prove to have IBD, particularly Crohn’s disease.43
Mild acute or chronic inflammation. A variety of pathogenic changes occur, which are similar to but much less marked than those seen in acute infectious colitis. These may be little more than an increase in chronic inflammation in the superficial half of the mucosa; focal changes in the luminal epithelium, which may be cuboidal or low columnar; and possibly occasional neutrophils in the epithelium, lamina propria, or mucosal capillaries. Sometimes differentiation from bowel preparation artifacts may be difficult.
Specific histologic pattern. Specific histologic features may be pathognomonic of some infections and may be of help in the differential diagnosis of others (Table 19-2). For example, pseudomembranous enterocolitis is most commonly associated with C. difficile infection. Verotoxin-producing organisms may also cause these changes, although the pseudomembranes tend to be more of a histologic finding rather than seen grossly; however, they may also be seen in ischemic bowel and occasionally have been reported in shigellosis and staphylococcal disease. The finding of granulomas besides Crohn’s disease raises a differential diagnosis of tuberculosis, fungal infection, syphilis, chlamydial proctitis, and Yersinia infection among many others. If the granulomas are associated with necrosis or caseation, Yersinia and tuberculosis need to be considered. The histologic characteristics of Yersinia infection are particularly striking, consisting of central stellate necrosis with numerous neutrophils surrounded by a cuff of palisading histiocytes. Occasionally, granulomatous lesions may be associated with M. avium-intracellulare infection, although in AIDS it frequently results in a diffuse infiltrate of foamy histiocytes, but lacking in other inflammatory cells similar to those in Whipple’s disease.
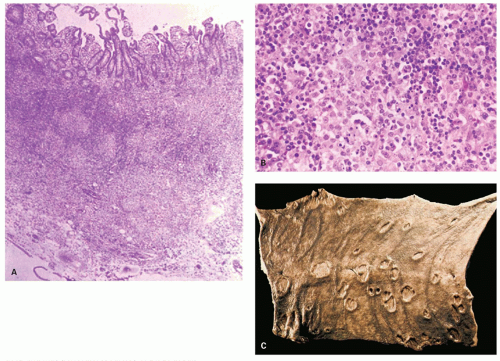
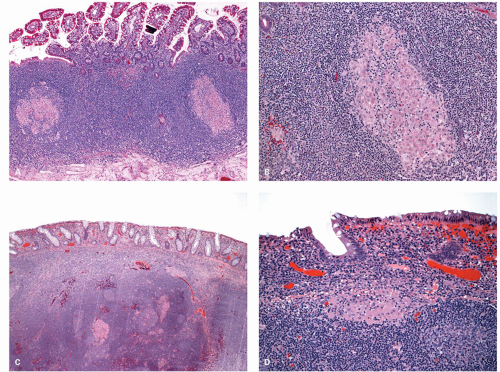
Typhoid fever has a fairly characteristic gross and microscopic appearance, although biopsies are rarely performed. Grossly, there is marked hyperplasia of gut lymphoid tissue, particularly of Peyer’s patches, producing raised longitudinal folds of mucosa that are superficially ulcerated and may perforate. Histologically, the lymphoid tissue contains aggregates of distinctive macrophages stuffed with ingested cellular debris, neutrophils, and erythrocytes, the so-called Mallory cells.
Detection of specific organisms or their cytopathic changes. In some cases, the cause of the enteric infection can be diagnosed because the offending organism or its characteristic cytopathic changes can be identified in tissue sections (Table 19-2). For example, a variety of protozoa, parasites, yeasts, bacteria, and fungi can be easily identified in tissue sections that include ameba, Giardia, Aspergillus, Zygomycetes, Strongyloides, Schistosoma, spirochetes, and so on. Some of the viral infections such as CMV, adenovirus, or herpes can be identified by typical nuclear or cytoplasmic inclusions. The identification of these organisms can be aided by ancillary methods that include histochemical stains, immunostains, in situ hybridization methods, electron microscopy, and PCR-based assays.
Special stains. A variety of histochemical stains that include tissue Gram stain, periodic acid-Schiff (PAS), Giemsa, mucicarmine, Fontana-Masson stain, acid-fast stains, and various silver impregnation methods are useful in highlighting various organisms. None of the stains are specific as they merely highlight the pathogens in some way; however, they are generally cheap compared to more advanced methods and are readily available in most labs. The commonly used histochemical stains used for specific pathogens are listed in Table 19-1 and also discussed under specific infections. A number of antibodies (monoclonal or polyclonal) have been developed for a large number of organisms that can be applied for immunohistochemical analysis on paraffin-embedded sections (Table 19-3). These are either commercially available or available at specialized centers like Center for Disease control in Atlanta, Georgia. In practice, only a few are available for everyday routine diagnostic use, even in tertiary care medical centers.
Table 19-3 Infectious Agents for Which Monoclonal or Polyclonal Antibodies or Both Are Available for Immunofluorescence or Immunohistochemistry
Bacteria
Fungi
Actinomyces
Aspergillus
Bartonella
Candida
Brucella
Cryptococcus neoformans
Clostridium
Histoplasma capsulatum
Campylobacter
Zygomycosis
Escherichia coli
Escherichia coli (O157:H7)
Mycobacterium
Neisseria gonorrhoeae
Salmonella
Shigella
Treponema pallidum
Vibrio
Protozoa
Cryptosporidium
Entamoeba histolytica/dispar
Giardia
Microsporidia
Toxoplasma gondii
Yersinia
Chlamydia
Coxiella burnetii
Ehrlichia chaffeensis
Rickettsia
Viruses
Adenoviruses
Cytomegalovirus
Epstein-Barr virus
Herpes simplex viruses 1 and 2
Human herpesvirus 8
Human papillomaviruses
Measles virus
Varicella-zoster virus
Electron microscopy. Electron microscopy is rapidly losing its popularity in the workup of infections and is seldom necessary in routine practice. However, in many academic centers, it is still performed for a variety of reasons, including identification of viral infections that do not produce typical cytopathic changes and many intracellular pathogens that are difficult to see on light microscopy (Cryptosporidia and microsporidia). Availability of various immunostains and molecular tests has gradually replaced electron microscopy for the identification of infections; however, occasionally a diagnosis of infection is first made on electron microscopy. Electron microscopy is also helpful as for some of the pathogens, especially viruses, reliable antibodies for immunohistochemical analysis are unavailable, and some of the intracellular pathogens are difficult to identify on light microscopy. Occasionally, one may also observe viral particles that remain unidentified and of unclear significance.
Molecular tests. Development of molecular techniques has redefined the approach to diagnosis of infections, especially for viral pathogens. These include in situ hybridization (Table 19-4) and PCR and other amplification-based assays (Table 19-5). Application of these techniques in surgical pathology for the diagnosis of infections is somewhat limited and available only at specialized centers. In situ hybridization is very commonly used in practice for human papillomavirus (HPV) and Epstein-Barr virus (EBV) infections, less commonly for CMV. This technique has the advantage that the pathogen may be localized to a specific cell type or an area on sections, similar to immunostains. PCR-based assays need to be interpreted carefully, as the tests will not differentiate between contaminants and true pathogens, or between integrated viral nucleic acid in a latent infection and active disease. However, these tests are highly sensitive and can be invaluable when cultures have not been obtained, when organisms in sections are sparse, or for organisms that are difficult or impossible to culture. The results can be obtained much quicker than cultures, especially for slow-growing organisms like mycobacteria. In situ PCR assays have also been developed that help to localize the reaction to specific areas of the tissues or cells; however, they also have limitations and are not yet widely available.
Gastrointestinal Infections in Specific Clinical Circumstances
Several modes of infection and clinical situations that imply a different range of expected organisms are listed below. These include several specific modes of infection (which are not mutually exclusive) including:
Table 19-4 Infectious Agents for Which DNA Probes for In Situ Hybridization Assays Are Available
BACTERIA
VIRUSES
FUNGI
Campylobacter
Adenoviruses
Aspergillus
Mycobacterium
Cytomegalovirus
Candida
Neisseria gonorrhoeae
Epstein-Barr virus
Cryptococcus neoformans
Rhodococcus equi
Herpes simplex viruses 1 and 2
Histoplasma capsulatum
Chlamydia
Human herpesvirus 8
Measles virus
Rotavirus
Human papilloma virus
Table 19-5 Infectious Agents for Which PCR Assays Are Available
Bacteria
Viruses
Fungi
Actinomyces
Adenoviruses
Aspergillus
Bartonella
Cytomegalovirus
Candida
Brucella
Campylobacter
Epstein-Barr virus
Pneumocystis jirovecii
Clostridium difficile
Escherichia coli
Escherichia coli (O157:H7)
Mycobacterium (others)
Mycobacterium tuberculosis
Nocardia
Salmonella
Shigella
Treponema pallidum
Tropheryma whippleii
Vibrio
Yersinia
Chlamydia
Ehrlichia chaffeensis
Rickettsia
Hantaviruses
Herpes simplex viruses 1 and 2
Human herpesvirus 8
Human papillomaviruses
Measles virus
Rotavirus
Varicella-zoster virus
Protozoa
Cryptosporidium
Entamoeba histolytica
Microsporidia
Toxoplasma gondii
1. Traveler’s diarrhea
2. Point outbreaks of infection
a. Foodborne illness
b. Temporary (or continuing) failure of the water supply and other waterborne infections
c. Institutionally acquired infection
i. Day care centers
ii. Nursing homes
3. Health care-associated (nosocomial) infection (HAI)
4. Oral-anal sexual practices
Traveler’s diarrhea. This is the occurrence of diarrhea when visiting or following a visit to a different geographic region, irrespective of whether or not international boundaries are crossed, and does not necessarily involve travel to high-risk areas, although the chances of getting diarrhea are high and in some countries approach 50%. Interestingly, a similar figure occurs in travelers from one developing country to another and the incidence has not changed over the years.44, 45, 46 Because 20% to 60% of visitors to developing countries develop diarrhea, these infections are generally known as traveler’s diarrhea, as well as a variety of colorful pseudonyms, such as Delhi belly or Montezuma’s revenge. High-risk areas include Asia, Africa, South and Central America, and the Middle East. Conversely, only about 10% of travelers to industrialized areas such as North America, Australia, or Northern Europe develop these diseases. Diarrhea is not uncommon when travelers from Europe visit North America or Japan, and vice versa, and even when traveling from one non-Western country to another. Similarly, travel within Europe or the North American continent is sometimes accompanied by a brief bout of diarrhea. Typically, these episodes occur following acquisition of local strains of E. coli, suggesting that habitants of that region acquire immunity to local organisms, while visitors may have to acquire it. Because organisms have to be ingested, they are acquired from either local water or food. A typical spectrum of organisms acquired as part of travelers’ diarrhea based on the geographic location is shown in Table 19-6.46 The unknown group likely includes organisms not yet recognized as being potentially pathogenic, a possible example being Campylobacter upsaliensis.47 Other viruses, which might not be found unless electron microscopic examination of stool is carried out, are also possible. In addition, infection with Giardia may not be manifest for weeks or months following infection.
Point outbreaks of infection. Localized outbreaks of infection are one of the most common sources of failure in communities in which water and sewage problems do not exist, although sometimes they may result from contamination of a local water supply. Disease may result from a variety of toxins that may be preformed or are elaborated from organisms that proliferate in the food. Pre-prepared and reheated or inadequately cooked foods are a major hazard; ingestion of fresh fish or shellfish is another potential source of infection. Despite quite stringent controls, common settings for all of these infections are restaurants, fast food outlets, cruise ships, airline food, and institutional food. Specific diseases are discussed in more detail in the sections covering particular organisms.
On a worldwide basis contaminated water is a major source of disease, typically caused by direct or indirect contamination of drinking water by sewage, but also associated with zoonotic contamination of drinking water. Major epidemics or pandemics, such as the pandemic spread of the El Tor strain of Vibrio cholerae, tend to occur in this setting. Spread is particularly likely to occur when river water is used domestically, as much natural sewage tends to drain into these sources. The use of water from local wells is a considerable advance, as it is far less likely to be contaminated due to the filtering of sediments in deep wells; shallow wells are more prone to contamination. Note that water used for washing fruits and vegetables and other raw or lightly cooked foods may be the source of infection in persons who do not drink the water.
Table 19-6 Identification of Specific Enteropathogens Shown as Percentage of Total Cases in Studies of the Etiology of Traveler’s Diarrhea Carried Out in Latin America/Caribbean, Africa, and Southern Asia, 1973-2004
PATHOGEN
L. AMERICA AND CARIBBEAN (%)
AFRICA (%)
SOUTH ASIA (%)
SOUTHEAST ASIA (%)
ETEC
33.6
31.2
30.6
7.2
EAEC
24.1
1.8
16.0
NA
EPEC
14.3
7.7
NA
18.0
EIEC
2.7
1.3
NA
1.03
EHEC
NA
0.5
NA
NA
DAEC
6.2
0
2.91
0
Campylobacter
2.5
4.6
7.82
32.4
Shigella
6.6
8.6
8.02
2.17
Salmonella
4.4
5.5
6.61
9.13
Aeromonas
0.8
3.2
2.81
3.27
Plesiomonas
1.3
2.5
5.41
4.78
Total vibrios
0.1
2.3
3.41
9.24
Noncholera
0.1
2.3
3.01
9.06
Vibrio cholera
0
0
0.4
0.18
Rotavirus
7.2
6.7
5.12
3.82
Norovirus
16.9
12.8
NA
3.17
Giardia
1.3
1.6
6.21
5.7
Cryptosporidium
2.0
1.3
2.81
0.63
E. histolytica/E. dispar
1.1
1.0
3.81
2.46
No pathogen identified
48.8
44.7
39.0
50.2
ETEC, enterotoxigenic E. coli; EAEC, enteroaggregative E. coli; EPEC, enteropathogenic E. coli; EIEC, enteroinvasive E. coli; EHEC, enterohemorrhagic E. coli; DAEC, diffusely adherent E. coli; Campy, Campylobacter, Crypto, Cryptosporidium; NA, organism was not sought in the studies.
Modified from Shah N, DuPont HL, Ramsey DJ. Global etiology of travelers’ diarrhea: systematic review from 1973 to the present. Am J Trop Med Hyg. 2009;80(4):609-614.
When an outbreak occurs, it is often possible to ascertain with a considerable degree of statistical certainty that a specific food, or sometimes beverage, was the source. Typically, this may be undercooked ground meat, shellfish, mayonnaise (uncooked eggs), unpasteurized milk or even fruits or vegetables washed with impure water, and a specific serotype of a particular organism is isolated. However, on occasion, the incriminated food or drink may be apparent from a statistical viewpoint, but all attempts to isolate an organism from either the food itself or the patients may fail to yield a pathogen, irrespective of the sophistication of the tests employed. Further, symptoms from these outbreaks may not be self-limited but may persist for months or longer (e.g., Brainerd-type diarrheas). It remains to be seen whether these represent new organisms or old organisms reemerging in a new guise.
Health care-associated (“nosocomial”) infection. Apart from the potential hazards of institutional food discussed in the preceding section, some infections may be transmitted between patients, presumably directly or via staff or visitors. In neonatal and pediatric units, viruses (rotaviruses and other enteric viruses) and bacteria such as enteropathogenic E. coli are particular causes for concern. In adult wards/units, C. difficile infections may be transmitted under similar circumstances, as may noroviruses (see the sections on these organisms).
Oral-anal sexual practices. These patients are susceptible to a variety of anorectal traumatic injuries as well as GI infections, and either may manifest as a proctitis or anal disease. Infections are common because of both the nature of the sexual practices and the number of sexual partners often associated with men who have sex with men, which facilitates transmission of both sexually transmitted and enteric pathogens. Multiple infections are common.48 Many of these infections and the part of the gut that they infest are summarized in Table 19-7. A major difficulty in this area is that there is a significant asymptomatic carriage rate of potential pathogens, such as Entamoeba histolytica/dispar and Campylobacter, and infection with multiple pathogens is frequent.40
Biopsies are usually not the first line of investigation in this group of patients unless a malignancy needs to be excluded. Biopsies are obtained once the initial workup is negative and diarrhea or proctitis remains unexplained, or an infection that is not easy to detect by culture or other noninvasive methods is being sought. Tumor-like lesions may prove to be a chancre, an ulcerated lesion of Chlamydia, ameboma, condyloma acuminatum, condyloma lata, or, rarely, neoplasms such as Kaposi’s sarcoma, lymphoma, or, in the perianal skin, verrucous or ordinary squamous carcinoma. In taking care to look for unusual infections, it is useful if the pathologist is aware that the patient is gay. An awareness of HIV infection or risk factors increases the likelihood of the pathologist’s taking extra time to ensure that unusual organisms, as discussed in Chapter 3, are not present. In addition to infections, trauma due to anal sexual practices is not uncommon and anal fissures, lacerations, and perirectal infections and abscesses are other lesions that can be seen in this population. Lesions usually or exclusively associated with AIDS are discussed in more detail in Chapter 3.
Table 19-7 Infections in Male Homosexuals and Sites of Involvement
aInfections primarily found in patients with AIDS.
bOther: These include several related amebae which are either nonpathogenic or of low pathogenicity, such as E. hartmanni, E. coli, Iodamoeba buetschlii, and Dientamoeba fragilis. They also include other nonpathogenic protozoa found more frequently in this population, such as Trichomonas hominis and Chilomastix mesnili.
There remains a minority of homosexual patients with proctitis in whom no infectious cause can be identified. Many of these conditions resolve with time. In those that do not, it is often difficult to rule out reinfection, repeated trauma, chronic infection with agents not yet recognized, or more classical idiopathic ulcerative proctitis, although biopsy can usually readily distinguish the last. About 25% of rectal biopsy specimens in homosexual men from whom no pathogen can be cultured show a chronic inflammatory infiltrate in the lamina propria40; in these cases, it is purely speculative whether this is the result of trauma or an occult infection.49 Although all of these diseases have been referred to as the syndrome of gay bowel disease,50 it is not really a syndrome; it is neither specific nor has a common etiology. Other than providing an all-embracing term, there is little use for it. Furthermore, it is potentially misleading, since women who engage in anal intercourse are also at risk.
ACUTE INFECTIOUS (SELF-LIMITED) COLITIS AND PROCTITIS
This is discussed at the outset as a separate entity as in vast majority of acute diarrheal illnesses, with or without blood, the specific cause is never found or vigorously pursued and these resolve spontaneously. Most of these never undergo biopsy; however, when they do, the range of histologic findings in the majority of these is virtually identical despite differences in pathogens. Because the natural history of these diseases is to resolve spontaneously, the term acute self-limited colitis is often applied to them. The concept is very useful, in part because the biopsy appearances are frequently so characteristic that the usual resolution is predictable even in the absence of an identifiable pathogen. However, in a proportion of patients, acute infections do not resolve spontaneously in the predicted manner, and at some point the etiology as well as the possibility of IBD becomes a serious concern leading to further workup, including biopsies. In some cases, the acute symptoms resolve but the patient continues to harbor the organisms and progresses to a carrier state. Others in whom pathogens either have cleared or were never found continue to have diarrhea and appear to progress to a postinfectious enteritis, colitis, or an entity called postinfectious irritable bowel syndrome, which may go on for months and sometimes years and may be quite debilitating. A small proportion of patients progress to a disease indistinguishable from either ulcerative colitis or Crohn’s disease. For all of these reasons, we find it difficult to accept the term self-limited colitis since, in a proportion of patients, albeit fairly small, the disease is not self-limited. The alternate term would be acute infectious-type colitis, or if a potential pathogen is found, acute infectious colitis. However, this is also not perfect as some cases that are histologically identical may be due to drugs. It is perfectly acceptable to use acute infectious-type colitis/self-limited colitis as the final diagnosis as this highlights both aspects of the underlying pathology.
Pathogenesis and Clinical Features
A variety of pathogens discussed subsequently in detail can cause identical clinicopathologic picture of acute colitis. These include Salmonella, Shigella, Campylobacter, Aeromonas, Plesiomonas, E. coli, and Edwardsiella, among many others. In the majority, the disease is usually acquired orally, either by ingesting raw, poorly cooked, or fecally contaminated food or beverages or by swimming in polluted water and presumably ingesting fecal bacteria. Some are acquired during travel (traveler’s diarrhea, discussed later), particularly to underdeveloped countries. In many patients there is no epidemiologic incriminating factor. Usually the disease is well recognized by the patient, producing a sudden onset of diarrhea, colic, nausea, and vomiting; however, the symptoms may persist, become unduly severe, and cause dehydration and hypovolemia, or may be accompanied by the passage of blood.
A variety of ancillary tests that include stool examination, stool culture, serology, enzyme-linked immunosorbent assay (ELISA)-based antigen detection assays, or PCR-based assays that aid in the diagnosis are available. Biopsy is reserved for a subset of cases where the diagnosis remains unclear despite initial workup or the possibility of IBD needs to be excluded.
Exacerbations of Inflammatory Bowel Disease
Infection may be superimposed on IBD resulting in exacerbations, or sometimes represent the initial presentation of IBD.51 Exacerbations of IBD may occur with numerous organisms, including Salmonella,51Campylobacter,52, 53C. difficile toxin,54Yersinia,52 CMV,55 and even Legionella.56 This is discussed further in Chapter 18.
Gross and Endoscopic Appearances
In general, the endoscopic changes in the infectious colitides are patchily distributed and are often less severe than anticipated from the patient’s symptoms. They are also extremely variable, depending on the organisms and the integrity of the host’s immune system.
Histology
A wide range of morphologic changes may be found (Fig. 19-1), ranging from minimal edema and congestion or a chronic inflammatory infiltrate. The inflammatory infiltrate is maximal in the luminal half or two-thirds of the mucosa and is characterized by neutrophils primarily in the lamina propria, that is, with relatively fewer crypt abscesses unless severe. However, if crypt abscesses are present, they tend to be more superficial, often small and poorly formed, and located in the mid or upper crypt.34, 35, 36, 37, 38, 39 If marked, there may be withering crypts superficially and also pointed crypts basally. Patchiness may be apparent if several biopsy specimens are taken. The major differentiating feature from IBD is a normal crypt architecture, although the crypts may appear pushed apart by edema and inflammation.57 Also, the basal plasma cell or lymphoid aggregates that characterize IBD disease are absent. Variable but uniform, mucin-depleted crypts that tend to point at the crypt bases rather than to be rounded (severe disease only) are seen. It has been suggested that in patients with severe disease, lamina propria hemorrhage, primarily pericryptal, may be present.58
When the colitis resolves, usually the mucosa returns to normal. Rarely, features are found in infection that may mimic those of IBD, the most important of which is architectural distortion with reduced numbers of irregularly spaced, irregularly shaped crypts with loss of parallelism, branching, and a tendency not to reach the muscularis mucosae. This may be seen following severe infection, which causes extensive mucosal destruction, such as with Shigella,41 pseudomembranous colitis, Campylobacter,42 syphilis, and Chlamydia infections.40) Some features are commonly seen in both infectious and ulcerative colitis, and are therefore of little value in the differential diagnosis. These include superficial epithelial destruction with exudate, diffuse mucin depletion, and crypt abscesses.
Diagnosis
Most forms of infectious diarrheas are self-limited and do not require specific forms of treatment other than fluid replacement, even when the specific organism is not identified. Thus, diagnostic studies are usually reserved for epidemics or local outbreaks or for cases with unusual features, such as:
1. Severe debilitating diarrhea, systemic complaints, and need for hospitalization.
2. Chronic diarrhea in which the differential diagnosis includes noninfectious etiologies such as IBD and less common forms of colitis such as ischemic or collagenous colitis.
Most clinical laboratories offer only a limited number of diagnostic tests (see approach to GI infections earlier). The diagnostic yield is generally low. If only three organisms are routinely cultured, namely, Salmonella, Shigella, and C. jejuni, the diagnostic yield from routine stool cultures is only about 8%. However, this rises to 15% in the presence of fever, bloody diarrhea, or both and to 46% with the additional finding of numerous fecal neutrophils. In contrast, reference and research laboratories are usually set up to detect over 20 agents. Their recovery rate of infectious agents of gastroenteritis is frequently over 50% and can be as high as 80% in certain risk groups, such as those with infantile diarrhea.20
BACTERIAL INFECTIONS
Vibrios
Vibrios are a group of motile, comma-shaped, gram-negative organisms responsible for a variety of infections. The most important of these by far is V. cholerae, which is responsible for cholera, although other variants, such as V. parahaemolyticus, are a well-recognized cause of gastroenteritis in some countries, such as Japan.59 In the United States, it is the leading cause of deaths associated with consumption of seafood in immunocompromised individuals, especially those with underlying liver disease.60
Epidemiology. Cholera is an important cause of diarrhea in many parts of the world and these episodes occasionally become pandemics. Every year, there are about 3 to 5 million cases of cholera worldwide resulting in about 100,000 to 120,000 deaths.61 The organism for cholera was discovered by Robert Koch in 1883 during an outbreak in Egypt.62 During the 19th century, cholera spread across the world from its original reservoir in the Ganges delta in India.63 Since 1817, so far it has resulted in seven pandemics, and it is believed that we are now in the eighth pandemic, which started as an epidemic in 1992 in Chennai, India, as a result of a new serogroup O139 (also called Bengal).64 This has apparently spread to about 13 countries in Southeast Asia. Most cases in the Untied states have resulted from travel to endemic areas, although toxigenic V. Cholerae O1 El Tor Inaba appears to have an environmental reservoir on the US Gulf Coast.65 In the United States, sporadic cases and few small outbreaks have been reported.66, 67 It seems that both variants are now pandemic.
Diseases caused by V. cholerae have two major biotypes, classic and El Tor. The classic has been responsible for the first six pandemics; the latter has been responsible for the seventh pandemic, which started in Indonesia in 1961. Fortunately, the El Tor results in a milder disease than that produced by the classic strain, from which it is easily separated by its ability to lyse sheep or goat red blood cells. V. cholerae can also be subdivided into three major O:1 serotypes (Inaba, Ogawa, and, rarely, Hikojima) with antisera, and into a further heterogeneous group of organisms of non-O:1 serotypes, which produce a variety of toxins that can also cause a wide range of infections including cholera and a dysentery-like illness.
Clinical features. After an incubation period of 24 to 48 hours, the symptoms begin with a sudden onset of painless watery diarrhea that rapidly becomes voluminous, often followed by vomiting.68 The stools have a “rice water” appearance and a fishy odor. Without fluid replacement, patients may develop dehydration followed by shock and death. Most individuals (75%) infected with V. cholerae remain asymptomatic, and most symptomatic patients have mild to moderate disease with spontaneous recovery. About 5% develop a severe form of the disease (cholera gravis) and with adequate treatment the mortality is <1%.
Pathogenesis. It is the prototype for enterotoxigenic secretory diarrheas. Disease follows ingestion of large numbers (probably at least 109) of organisms in food or contaminated water, and is facilitated by partial gastrectomy or hypochlorhydria of any cause, probably by decreasing killing by gastric acid.6 Colonization likely occurs following entrapment of the organisms in the mucous layer,27 which occurs mainly in the duodenum and jejunum. Following colonization, toxin is introduced into the cell.
Cholera toxin acts by permanently activating cyclic adenosine monophosphate (AMP), which results in persistent electrolyte secretion; the cascade mechanism has been relatively well elucidated 69 The toxin is an 84-kD protein consisting of a ring of 5 B subunits surrounding a single A subunit.70 The B subunits bind to a GM1 ganglioside receptor on small intestinal epithelial cells, and the A subunit is “injected” into their cytoplasm. Here it is cleaved on the inner cell membrane, forming A1 and A2 fragments. Within the enterocytes:
1. Electrolyte secretion is controlled by cyclic AMP.
2. The activity of cyclic AMP is controlled by adenylate cyclase.
3. Adenylate cyclase activity is controlled by adenosine monophosphatase guanine triphosphatase (GTPase).
4. GTPase is controlled by levels of ADP-ribose.
5. ADP-ribose results from the breakdown of nicotinamide adenine dinucleotide (NAD) to nicotinamide and ADP-ribose.
The cholera toxin increases the level of ADP-ribose in cells because its A1 fragment catalyzes the breakdown of NAD. Thus, the A subunit of cholera toxin is cleaved within enterocytes to form A1 and A2 fragments. The A1 subunit catalyzes the production of ADP-ribose from NAD. ADP-ribose controls GTPase, which in turn maintains adenylate cyclase in an active state, thereby causing the enterocyte to permanently secrete electrolytes.71 Although it was initially thought that small intestinal secretion was so great as to overwhelm colonic absorptive activity, decreased colonic absorption also potentiates the disease.72 It should also be remembered that secretion in the small bowel takes place primarily in the crypts, so that there is probably an additional effect preventing the activation of absorptive cells in the villi.
Following infection, antibodies develop both to somatic antigens on the bacillus and to its toxin, strongly suggesting that both the organism and its toxin reach the immune cells of the lamina propria. There is evidence that this occurs through active ingestion of organisms in the M-cells overlying Peyer’s patches and lymphoid nodules.73
Pathology. Light microscopy produces unremarkable results. Although several publications have suggested an increase in mononuclear cells in the lamina propria of the small bowel, to date we are unconvinced that this represents anything but background inflammation similar to that seen in the local population; only occasional subepithelial edema and a little congestion/hemorrhages suggest that the mucosa is abnormal.74, 75 This results in morphologic changes that are largely ultrastructural with irregular widening of intercellular spaces and junctional complexes. On the surface of the enterocyte, organisms disrupting microvilli are visible. Large cytoplasmic processes may also project into the lumen.76 Studies in experimental animal also show structural changes in the villous architecture and infiltration by inflammatory cells.77
Diagnosis. Diagnosis can be established by directly demonstrating the organisms that exhibit typical “shooting star” motility in the stool by dark field illumination. The organisms can be isolated using selective media. PCR-based assays for toxin identification that can help in rapid diagnosis are also available.78, 79
Treatment and follow-up. Therapy consists primarily of rehydration with sugar and salt solutions to overcome the loss of fluid and electrolytes.68 Mortality is highest in those patients who are least able to tolerate fluid loss, namely, the very young, the very old, and those with other debilitating illnesses. Vaccines with short-lasting effects are also available.80
Escherichia coli
Escherichia coli (E. coli) was first described by Theodore Escherichia in 1885.81 These are gram-negative, short (1-5µm), straight or occasionally slightly curved, bacilli that are ubiquitous in the environment, colonize the human gut within hours of birth, and play an important role in maintaining gut physiology. They form the normal gut flora of warm-blooded animals and humans; however, some organisms have acquired virulence factors and have become pathogenic.82 The pathogenic E. coli can be diarrheagenic or nondiarrheagenic (uropathogenic or meningitis associated). Diarrheagenic E. coli is a common cause of intestinal infection worldwide. Based on virulence properties, pathogenic mechanisms, distinct serogroups/serotypes, and clinical syndromes they have been separated into six different pathotypes, namely, enterotoxigenic (ETEC), enteroinvasive (EIEC), enterohemorrhagic (EHEC), enteropathogenic (EPEC), enteroaggregative (EAEC), and diffusely adherent or enteroadherent (DAEC) E. coli.83 Usually specific but different serotypes regularly seem to cause the same type of infection mechanistically. The various pathotypes and the common clinical syndromes are given in Table 19-8.
Table 19-8 The Various Pathotypes and the Common Clinical Syndromes Associated withE. coli
TYPE OF E.COLI
MODE OF TRANSMISSION
MECHANISM
CLINICAL FEATURES
Enterotoxigenic
Humans
Heat stable or heat labile enterotoxin
Infantile and travelers diarrhea
Enteroinvasive
Food borne or water borne, humans
Tissue invasion and intraepithelial proliferation
Dysentery or nonbloody diarrhea
Enterohemorrhagic
Food borne
Shiga toxins, and attaching and effacing lesions
Hemorrhagic colitis and HUS
Enteropathogenic
Humans
Attaching and effacing lesions
Infantile diarrhea
Enteroaggregative
Food borne
Adherence, enhanced mucus production and EAEC cytotoxin
Diarrhea in children and adults
Diffusely adherent
Food borne
?
Diarrhea in young children (1-5y)
EnterotoxigenicE. coli. These organisms are a frequent cause of traveler’s diarrhea and cause disease by adhering to and colonizing the upper bowel. They produce a variety of toxins, including the heat-labile and heat-stable cholera toxins. These toxins have a well-elucidated mechanism of action in stimulating adenyl cyclase activity, causing a severe secretory diarrhea with relatively little morphologic abnormality (see previous section).
EnteroinvasiveE. coli. This group of E. coli organisms emulates the traditional organisms that typically cause acute infectious diarrhea, such as Shigella, Salmonella, or Campylobacter. Indeed, the similarities between Shigella and these strains of E. coli are so great that they are clearly closely related, and separation is somewhat artificial. They also produce Shiga toxin, which appears to be dependent on the acquisition of the same plasmid, and similarly causes a dysentery-like illness primarily affecting the large bowel.84 The diagnosis is made by serotyping suspect E. coli strains by an ELISA method detecting outer membrane proteins, or by DNA hybridization techniques using probes for the genes for invasiveness.28 Because these methods are not routine in many laboratories, the organisms are likely to go undetected most of the time. The morphology of infection is poorly documented, and likely produces an infectious (acute self-limited) colitis that may be indistinguishable from some Shigella infections.41
Enteropathogenic organisms. This is initially a confusing term that was (and still is) applied only to E. coli associated with infant diarrhea, which did not produce the cholera-like, heat-stable and heat-labile toxins that characterize other ETEC, and did not have the Shigella-like invasiveness of enteroinvasive organisms or the verotoxin production of EHEC.85 Nevertheless, feeding of these strains to volunteers produced diarrhea.86
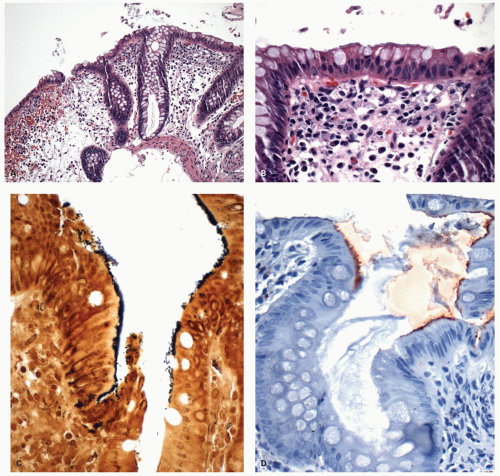
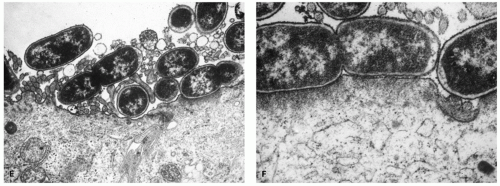
In affected infants, enteropathogenic E. coli are characterized by a distinct morphologic mechanism detected by electron microscopy in which organisms attach to and colonize the luminal border of the enterocyte, causing effacement of the microvilli and partially indenting (or being partially surrounded by) the cell membrane but leaving a gap of about 10 nm between the bacterium and cell membrane.85 This appearance is known as attachment/effacement, cupping, or pedestal formation (Fig. 19-2E,F).28, 87 It soon became apparent that chronic, as well as acute, infant diarrhea could be caused by similar E. coli organisms using an identical mechanism, and that the infection and symptoms could be terminated by antibiotics retaining their activity in the intestine.88
A large proportion of these organisms also adhere to cells of the HEp-2 cell line in a localized as opposed to diffuse manner, a property that allows the diagnosis to be made without the need to resort to biopsy and electron microscopy.
EnteroadherentE. coli. The possibility that some E. coli can cause diarrhea, yet either do not adhere to HEp-2 cells or adhere to them in a further definable manner, exists, and some have suggested that these be called enteroadherent E. coli (EAEC) (Fig. 19-2A-F).28 Such plasmid-free strains are able to cause the typical, attachment/effacement of microvilli seen on electron microscopy and clinical diarrhea, but they may be less efficient than their plasmid-containing counterparts. In one study, 30% of patients acquiring diarrhea abroad had these organisms compared with 8% in healthy individuals.89 The ability of these organisms to produce these lesions in culture with small intestinal enterocytes attests to their pathogenic potential.90 Nevertheless, some strains of E. coli causing infant diarrhea do so in the absence of in vivo enteroadherence or the demonstration of bacterial attachment to duodenal or rectal biopsy, specimens, raising the question of whether another mechanism of pathogenicity is present or whether in vivo and in vitro methods of demonstrating pathogenicity are inadequate, or both.50
Figure 19-2. Example of enteroadhesive E. coli in a biopsy. A: At low magnification one can see a fuzzy basophilic layer of organisms sticking to the surface mimicking appearance that is similar to intestinal spirochetosis. The remaining biopsy appearance is within normal limits with lack of any inflammatory infiltrate or mucin depletion of crypts. B: On closer look the organisms are shorter and hence the fuzzy layer appears thinner compared to intestinal spirochetosis. C: A Warthin-Starry stain highlights the thick coat of the organisms adherent to the luminal surface of the enterocytes; however, at this magnification one can appreciate that the organisms are rod-shaped bacteria rather than spirochetes that are longer and wavy. D: A polyclonal antibody for E. coli highlights the layer of organisms as well and can be used to further differentiate this from spirochetosis.
EnterohemorrhagicE. coli. These verotoxin-producing organisms are becoming an increasingly important cause of diarrhea, particularly hemorrhagic colitis. They may also be the cause of bloody diarrhea in about 15% of patients, and are second only to Campylobacter as an enteric pathogen in children in some series.91 In one statewide study from United States, the mean patient age of 93 isolates in 1 year was in the early teens, and the highest attack rate was in children under 5 years; 95% of patients had bloody diarrhea, and 12% developed HUS or TTP, but with only one death.92 The pathogenesis of verotoxin-producing organisms has been discussed previously.
Figure 19-2.(Continued)E: Electron micrograph of enteropathogenic E. coli in the jejunum, with typical attachment-effacement of microvilli (pedestal formation). F: Detail shows the loss of microvilli immediately beneath the attachment sites of the organisms. (Electron micrographs courtesy of Dr. Brian West.)
Infection occurs in isolated cases, but also in institutions such as day care centers or nursing homes, and has an incubation period averaging 3 to 4 days; particularly in the elderly, there may be a mortality of over 30%, frequently associated with the HUS or TTP.93, 94, 95, 96, 97 Patients taking (or treated with) antibiotics and older patients may be at increased risk, if only because the most severely ill patients may be given antibiotics that may suppress other organisms allowing proliferation of pathogenic strains. Secondary infection likely occurs from person-to-person spread, which may involve staff responsible for meal preparation, and by the fecal-oral route. Investigation is often precipitated by bloody diarrhea or by outbreaks of diarrhea in institutions.98 Intragastric infection in animals with verotoxin-producing strains of E. coli experimentally results in colonic disease with diarrhea and features of an acute infectious-type colitis and attachment of organisms to the luminal epithelium.99, 100
Clinical Features This disease typically begins with diarrhea that is profuse and watery, but the stool frequently becomes bloody, sometimes consisting almost entirely of blood. It is invariably associated with abdominal colic and sometimes with vomiting, but rarely with pyrexia.
Gross and Endoscopic Appearances Barium studies may show an appearance resembling that of ischemia, with thumbprinting that has a distinct tendency to occur in the right colon (Fig. 19-3B,C). These studies are rarely performed in an era where endoscopy is widely available. Endoscopy may show similar segmental disease, usually with redness and swelling (Fig. 19-3A),93 and increasing degrees of duskiness most marked in the right colon, with gradual distal sparing.101 In the most severe cases, the lumen may be virtually obliterated and the mucosa is dissolved, with patchy, shallow ulcers often covered by a yellow or green exudate. The submucosa is diffusely hemorrhagic, and this may also cause black discoloration of the serosa. The extent of colon affected in this way can vary, but the right colon is always affected, with a variable amount of the more distal colon in continuity. In contrast, the terminal ileum is often unaffected, allowing distinction from arterial occlusion102; however, the disease may be an enterocolitis, so that in severe cases coming to resection or autopsy, the small bowel including the terminal ileum can be severely affected.103 Rarely, in severe cases there may be pseudomembrane formation and ultimately ischemic infarction.97, 104, 105
Histology Although this disease is primarily a colitis, virtually any part of the GI tract can be affected, the small intestine being the next most severely affected site.103 A spectrum of changes may be seen histologically, varying from edema to subepithelial and lamina propria hemorrhage with fibrin deposition, which often dominates the histologic picture (Fig. 19-3D-G). Nonspecific inflammation or neutrophils may be present in the lamina propria, and it may have an appearance typical of acute infectious (self-limited) colitis. IgG-containing plasma cells may predominate in the upper lamina propria.102 In the most severe cases, there may be microulceration with coagulative necrosis of the upper mucosa,100 or all of the characteristics of pseudomembranous colitis may be present, with microvascular thrombi and ultimately sloughing of most of the mucosa (Fig. 19-3D-G).101, 102, 104, 105, 106 The latter is of interest in that the pseudomembranes tend to be more apparent histologically than endoscopically; the unexpected finding of histologic pseudomembranous colitis should therefore cause underlying verotoxin-producing E. coli to be suspected.97, 101, 102, 103, 104, 105, 106 The right-sided predominance of this disease should always be remembered in patients in whom examination and biopsy have been limited to the left colon or in whom multiple colonoscopic biopsy specimens reveal primarily right-sided disease. Rarely the disease may closely mimic Crohn’s disease, and testing of the organisms in stool and successful resolution of the disease following appropriate treatment is the only way of establishing the correct diagnosis.107 Otherwise, in IBD patients in whom these organisms are associated, the biopsy changes are of underlying disease.105
Figure 19-3. Enterohemorrhagic E. coli.A: Endoscopic appearance of verotoxin-producing E. coli colitis. B, C: Autopsy specimen with severe hemorrhagic and necrotizing disease. (Courtesy of Dr. L. Eifus.) D-G: Biopsies of verotoxin-producing E. coli.D: Low magnification of a biopsy specimen that reveals areas of lamina propria hemorrhage, mucin-depleted crypts and surface epithelial loss. The features resemble ischemia, with withered and mucin-depleted crypts along with eosinophilia and hyalinization of the lamina propria. The parallel orientation of the crypts is generally preserved. E: Another biopsy with similar features but also a hint of pseudomembrane formation is present. F: Higher magnification to show that besides pseudomembrane the other features are similar to ischemia. The pseudomembrane formation when present is often a histologic rather than an endoscopic finding. G: Detail of another biopsy showing lamina propria hemorrhage, which sometimes may be the most prominent finding.
Hemolytic uremic syndrome and thrombotic thrombocytopenic purpura. HUS is characterized by acute renal failure, thrombocytopenia, and microangiopathic hemolytic anemia, with elevated levels of fibrin degradation products and platelet and fibrin deposition in glomerular capillaries with underlying endothelial damage.106, 108 TTP is closely related and includes, in addition, neurologic sequelae and fever.97, 104 Although verotoxin-producing E. coli are by far the most common organisms predisposing to these diseases, numerous others have been postulated, primarily bacteria, including Shigella, Salmonella, Campylobacter, and Yersinia, but also viruses such as arbovirus, myxovirus, Coxsackie viruses, and enteric cytopathic human orphan virus.109 Also included, strangely, are cytotoxic drugs such as cisplatin, for reasons that are unclear.110 Many of these reports predated verotoxin detection, and many patients developing this syndrome have at least transient diarrhea, which may be bloody. Because these organisms also seem to produce the closely related Shiga toxin and appear capable of severely damaging endothelial cells, it is unclear whether both are required for the disease. The rarity of reports of HUS associated only with Shiga toxin-producing organisms alone suggests strongly that verotoxin is implicated.
Verotoxin-producingE. coliin inflammatory bowel disease. Numerous organisms have been associated with exacerbations, and possibly initiation (see also Chapter 18) of IBD, and appear to produce disease, which by histologic anecdotes tends to resemble the underlying disease rather than an acute infection. Verotoxin-producing E. coli are included in this list,105 and one unconfirmed report suggests that this may be with serotype O2:H5 rather than O157:H7 in some patients; it is also indistinguishable clinically from the underlying disease but responds to antibiotics.111
Shigella
Shigellosis affects the colon and causes severe bloody diarrhea (dysentery), of which it is a major cause worldwide; it is associated with 10% to 20% of all infective diarrhea.112 Humans are the usual reservoir. Shigella are virulent gram-negative bacilli; detection in the stool is usually associated with disease, and a carrier state is relatively uncommon. Serologically, four species (and numerous serotypes) can be identified: Shigella dysenteriae (serotype I of this group being S. shiga), S. flexneri, S. boydii, and S. sonnei.113 All are enteroinvasive and extremely closely related to EIEC. In the last few decades, S. shiga has gained the reputation of being more virulent than the other strains and has been the cause of severe epidemics in the developing countries. S. sonnei tends to be the mildest and, in the Western world, the most common isolate, accounting for about two-thirds of shigellosis in the United States. The disease is more common in underdeveloped or developing countries where living conditions are poor and sanitation is inadequate.
Pathogenesis.Shigella is usually ingested from fecally contaminated water. In large bowel the bacteria appear to induce their own endocytosis to gain access to epithelial cells, in which they replicate massively within colonic epithelial cells, apparently without damaging them before invading the lamina propria. This is followed by a diffuse desquamation of the mucosa in an exudate also containing abundant neutrophils and red blood cells.114 However, invasion into the bloodstream seems not to occur. The severity of the infection is presumably determined by the virulence of the particular organism, the host response, and possibly the number of infecting organisms. In addition to being invasive, many strains produce an enterotoxin that promotes secretion and may therefore explain the watery diarrhea that many patients experience.115, 116 This toxin causes reduced protein synthesis in the mucosal epithelium, while the bacterial endotoxin causes mitochondrial damage leading to cell death. Exposure of the endothelium to the toxin can also cause injury resulting in thrombosis of small vessels and subsequently ischemia. The pathogenesis of shigellosis is therefore in marked contrast to that of cholera, in which a secretory diarrhea occurs with relatively little morphologic abnormality; microscopic examination of the stools for the presence of neutrophils therefore readily distinguishes between these two diseases.
Clinical features. Endemic disease primarily affects debilitated and malnourished individuals, infants, and young children.117 In the latter two groups, there may be a heavy mortality, particularly in those who are already malnourished. In an epidemic in West Bengal in 1984, 78,000 cases of S. dysenteriae were reported in 4 months, with 2,200 deaths.41 Outbreaks are seen in crowded places of living in underdeveloped countries that include nursing homes, day care centers, and prisons. Infection usually follows contamination of the local water and oral ingestion. Person-to-person transmission also occurs, primarily as a sexually transmitted disease. In the United States there has been an increase in sexually transmitted shigellosis in the homosexual population.48
The organisms are amongst the most infectious of all gram-negative enteric bacteria and only 10 to 100 organisms are required to result in clinical disease. The incubation period is about 12 to 50 hours, and classically it manifests with colicky lower abdominal pain, fever, and watery diarrhea followed by bloody diarrhea. The disease may persist for periods ranging from a day to several weeks and responds well to appropriate antibiotics.
Complications include dehydration, toxic megacolon, Reiter’s syndrome reactive arthritis, and HUS.118 As with all severe colitides, fulminant disease can result in perforation, although this is quite uncommon.119 Carrier states unassociated with symptoms are very uncommon and tend to last for only a few months. Persistent disease has been reported but is rare.120 Respiratory and neurologic symptoms can occur and may even dominate the clinical picture in some patients.
Gross and endoscopic appearances. Early descriptions of this disease were made at autopsy, when it affected the entire large bowel and the disease was severe. In such cases, mucosa is diffusely hemorrhagic, with numerous patches of pus on the surface that may become confluent and form a pseudomembrane.121, 122 Rectum and sigmoid are most commonly involved. In a notable colonoscopic series from Bangladesh in which saline enemas were used for bowel preparation until clear showed that three-quarters of the isolates were S. flexneri and 15% S. dysenteriae, all patients had involvement of the rectosigmoid; it reached the splenic flexure in 55%, the midtransverse colon in 42%, the hepatic flexure in 27%, and the cecum in 15%.116 The extent seemed related more to the duration of the disease than to the underlying subtype. Further, 15% of the patients had lesions that were described as “aphthoid ulcers.”123 Involvement may stop abruptly at the ileocecal valve or, in patients with severe large bowel disease, may be present in the terminal ileum, thereby resembling Crohn’s disease.
Histology. In the West, milder cases, usually those associated with S. sonnei, have the typical appearance of an acute infectious-type colitis and are indistinguishable from other enteric infections. In severe disease, the superficial lamina propria is purulent, with numerous, primarily superficial, crypt abscesses. There may be a volcano-like pseudomembrane, marked mucin depletion, and distortion of the normal crypt architecture or colitis cystica superficialis (Fig. 19-4). This may resolve to leave an atrophic mucosa indistinguishable from that seen in quiescent ulcerative colitis.41 Perforation occurs in the setting of fulminant colitis with or without toxic dilatation, and with all the features of fulminant colitis, with “melting” of the submucosa and muscularis propria and subsequent peritonitis. Electron microscopically, apart from epithelial damage, there may be endothelial damage, with degranulation of eosinophils and mast cells.124
Diagnosis, differential diagnosis, and treatment. Milder disease may resolve spontaneously with supportive therapy; however, appropriate antibiotics may shorten the disease and are required for severe disease. Diagnosis is established with stool culture. The organisms are fastidious and rapidly die and hence need to be inoculated into culture media immediately. The disease needs to be differentiated clinically and pathologically from other gram-negative enteric infections (E. coli, Salmonella, etc.), C. difficile, and IBD. Although antibodies for IHC that are specific for E. coli and E. coli (O157:h7) are available, they are used sparingly for routine diagnosis. Similarly, molecular tests are also available, but seldom required in routine diagnostic workup.
Salmonella
Salmonella are gram-negative bacilli that cause enterocolitis, food poisoning, and typhoid (enteric) fever.112, 125 They are also an important cause of traveler’s diarrhea.46 However, Salmonella may also involve a variety of other organs, often individually, as in osteomyelitis or even septicemia, with or without evidence of enteric disease. The carrier state is also well defined, primarily for S. typhi. Salmonella infections are widespread and are transmitted through contaminated food and water. The organisms can survive partial cooking, freezing, or drying. Various food or food products that may contain these organisms include dairy products, eggs and egg products, meat, and vegetables.126 Patients with HIV infection are at increased risk of developing the infection, and so are patients with reduced gastric acidity.127, 128 The organisms can survive and multiply within Schistosoma parasites and patients with schistosomiasis are at a higher risk of infection with Salmonella, which may be recurrent.129
Figure 19-4.Shigella of varying severity. A: Marked acute inflammation causing superficial mucosal destruction. B1,B2: Features of acute infectious colitis, but with mild architectural distortion and pus in the lamina propria. C,D: Marked mucosal destruction, with colitis cystica superficialis in Shigella flexneri infection. E: The previous patient following resolution of the disease, showing marked residual architectural distortion.
Classification ofSalmonella. The three species of Salmonella that may be encountered are S. typhi (one serotype), S. cholerae-suis (two serotypes), and S. enteritides, of which there are close to 2,000 serotypes. In practice, growth characteristics and identification of the Vi antigen (S. typhi only), and of somatic (O) and flagellar (H) antigens, sometimes at reference centers, are required for complete identification. The most important species and subgroup are S. typhi, S. cholerae-suis, and the three major serotypes of S. enteritidis, formerly referred to as paratyphoid A, B, and S. typhimurium, but now called S. enteritidis bioser Paratyphi A, S. enteritidis ser Paratyphi B, and S. enteritidis ser Typhimurium.
Although typhoid fever is usually caused by S. typhi, this and both paratyphoid A and B invade the bloodstream, causing “enteric fever.” S. cholerae-suis may also do so, but primarily in children; usually it causes a gastroenteritis. Over 70% of Salmonella isolates are associated with enterocolitis. The most common isolate was once Typhimurium, although in many centers others, such as S. hadar, are now the most frequent (see below). The new isolates tend to be referred to by the region, town, city, hospital, or patient from which they were isolated. Enterocolitis is associated with many of them, although some are so well adapted to a specific animal that infections in other animals or humans are rare.
Also of interest is the similarity between human and animal isolates; S. typhimurium usually heads both lists and illustrates the relative ease with which animal strains are transmitted to humans. This is perhaps best exemplified by S. hadar, which was the second most common isolate in England for several years in the early 1980s. The reservoir appeared to be turkeys, contamination of which was associated with about one-half of the cases.130 Similarly, S. agona was introduced into pigs and poultry as a contaminant of fish meal from Peru; this strain also rapidly climbed the human isolate listings. Thus, the association of food, fingers, feces, fomites, and flies remain the modes of spread.
Salmonella enterocolitis.Salmonella is one of the most common foodborne pathogens.131 Despite the numerous serotypes of Salmonella, in most countries a handful of serotypes account for most of the infections. Most outbreaks result from contamination of food or meal at the time of production that are distributed widely in the community. These include contamination of chocolate (S. eastbourne), carmine dyes (S. cubana), hamburger and precooked roast beef (S. newport),132 powdered milk (S. newbrunswick), and marijuana (S. muenchen),133 as well as raw milk (S. dublin)134 and turkey (S. hadar),130 pigs (S. agona), poultry and eggs, and phage type 4.135, 136 An unusual outbreak of S. eimsbuettel in neonates appears to have been spread by rectal thermometers.137
Clinical Features Most patients have gastroenteritis of varying degrees of severity, with a severe bloody diarrhea leading to dehydration and, rarely, toxic dilatation and perforation; at the other extreme, minor diarrhea lasting for 24 hours or less occurs. Some patients who have clearly eaten contaminated food do not develop any disease. Treatment with antibiotics is not recom-mended except in potentially life-threatening situations because of the increased likelihood of producing a carrier state. Conversely, patients traveling to areas where there is a high likelihood of acquiring enteric pathogens can markedly reduce their chances of acquiring other infections with prophylactic antibiotics, but may increase the risk of developing salmonellosis.138
Endoscopic Appearances The changes can be diffuse or patchy. Typically mucosa is erythematous and friable. It may extend for a variable distance proximally and mimic ulcerative colitis. While rectal involvement is usually present, the preferential involvement of the proximal colon strongly favors Salmonella colitis. Some patients from whom Salmonella is isolated have no endoscopic abnormality and may be carriers.
HistologySalmonella produces the same range of changes as other types of acute infectious colitis (Fig. 19-5).139 Patients with no endoscopic abnormality may have no histologic abnormality. When minimal changes are present, the main features are little to none, goblet cell mucin depletion, edema, and a neutrophilic infiltration in the lamina propria that tends to be crypt sparing. In virtually all cases there is preservation of the normal crypt architecture, but separation of the crypts from each other and often from the muscularis mucosae because of mucosal edema. Basal lymphoplasmacytic aggregates are conspicuous by their absence. The increase in the inflammatory infiltrate varies from slight to marked.
With more intense inflammation the appearance resembles an acute infectious type colitis. The changes include attenuation or erosion of the surface epithelium, partial or complete depletion of crypt mucus, and focal accumulations of neutrophils in the lamina propria that are almost purulent, with crypt abscesses, often lined by attenuated epithelium, primarily in the upper halves of the crypts and sometimes pointing to the crypt bases. Neutrophils may also be present in the surface epithelium and in lymphoid follicles, if present.140, 141S. typhimurium also produces an acute diffuse colitis with similar histology, but autopsy cases have demonstrated acute inflammation of the small intestine, as well as one instance of acute gastritis in a patient with a partial gastrectomy; the H. pylori status was not given.139 There is more overlap between the pathology of nontyphoid Salmonella species with typhoid-producing Salmonella than is generally recognized.
Figure 19-5.Salmonella colitis with typical appearance of an acute infectious colitis, with an excess of inflammation but little inflammation at the muscularis mucosae and no crypt distortion.
Destruction of the superficial part of a crypt results in the formation of a crypt abscess that extends beyond the limit of the original crypt. Re-epithelialization of the original crypt and the boundary of the abscess may therefore result in bifid or irregular crypts. Biopsy specimens taken during the resolving phase of the disease or following resolution may therefore show minor architectural disorganization that is usually limited to the superficial part of the affected crypt. When severe infection has occurred, usually with S. typhimurium, crypt destruction during the acute phase of the disease may be sufficient for follow-up biopsy to produce an architectural change similar to that seen in quiescent ulcerative colitis.140, 141 The same is frequently true of Shigella infections.41 Rarely, the acute phase may produce the appearance of colitis cystica superficialis.
Fulminant infections. These include a hemorrhagic, edematous mucosa in which transverse ulcers are focally apparent. Architectural abnormality is sometimes present in residual mucosa, particularly when severe inflammation is present. The most severely affected mucosa may be bereft of crypts, with hemorrhage and fibrin being present in both the mucosa and the submucosa; platelet thrombi may also be present in capillaries in the submucosa and may extend into the small venules. Neutrophils are the predominant cell type in both the mucosa and the submucosa.141 Rarely toxic megacolon can be seen with Salmonella colitis.142
Salmonellainfection in inflammatory bowel disease. Despite a possible association between these two conditions, which some have questioned,51 and the possible predisposition of patients with ulcerative colitis to develop salmonellosis when treated with steroids, the biopsy appearances of the combined diseases are not well described despite the clinical need for therapeutic reasons. To date, the reports discussing histology suggest that the appearance of active ulcerative colitis with Salmonella is that of ulcerative colitis,36, 140 while in Crohn’s disease it may resemble infection with neutrophils primarily in the lamina propria, with relative crypt sparing.140 This resembles our experience with infections in ulcerative colitis. However, it is becoming increasingly apparent that a crypt-sparing neutrophilic infiltrate in the lamina propria may be seen in both Crohn’s disease and infection, and this is unhelpful in their distinction. In addition, both diseases may share focality of the inflammatory process and a tendency to involve the right colon, primarily when the underlying infection is Salmonella or Yersinia. Salmonella does not seem to produce focal disease with ulceration on one side of a biopsy and a relatively normal appearance on the other side, which is typical of aphthoid ulcers in Crohn’s disease. Nor is severe focality present between biopsies or a deep lymphoplasmacytic infiltrate present in salmonellosis.
The diagnosis of Salmonella infection is established with stool cultures, or culture of blood or bone marrow in case of typhoid fever.
Typhoid fever. This is usually caused by ingestion of typhoid (S. typhi) or paratyphoid (S. enteritidis serovar Paratyphi A and S. enteritidis serovar Paratyphi B) organisms and results in a variety of systemic manifestations, abdominal pain (often in the right lower quadrant), splenic enlargement, fever, and the classic rose spots in the skin.
Pathogenesis and Clinical Features. This is a disease of all ages, although there tends to be a peak in the third decade and often a male preponderance.143 The organisms penetrate the small intestinal mucosa, apparently without inducing a host response, and rapidly gain access to lymphatics, lymph nodes, and the bloodstream to reach macrophages throughout the body, where they multiply (incubation). Histiocytic nodules form in a variety of tissues, and there is marked hyperplasia of lymphoid tissues.144 Between 1 and 2 weeks later, organisms are released into the bloodstream, initiating symptoms (acute invasion). Symptoms are maximal during the 3rd week, corresponding to necrosis of lymphoid tissue and toxin release (fastigium), with high, swinging fever, mental confusion, and “peasoup” diarrhea. Symptoms gradually resolve about the end of the 4th week (lysis), when the patient is weak and tired but has no other symptoms (convalescence). Because S. typhi is an exclusively human disease, the presence of a case implies a human carrier, who in many countries requires identification.
The most severe complications are intestinal hemorrhage and perforation, both of which occur in or from Peyer’s patches.145 Acute cholecystitis can occur during the 2nd or 3rd week, and the gallbladder may remain infected for long periods, particularly in elderly women with gallbladder disease. After 3 months, organisms are still excreted by 5% to 10% of patients; the chronic carrier state is by definition isolation of the organism 1 year after the onset of symptoms or persistent excretion for a year in patients who are asymptomatic. Chloramphenicol is often the drug of choice, and symptoms abate 3 to 5 days after therapy is started.
Gross Appearance There is a diffuse enterocolitis characterized by dilatation and redness of the small intestine; hyperplasia of lymphoid tissue is prominent, individual lymphoid nodules being raised above the adjacent mucosa and ulcerated (Fig. 19-6). The appendix may also be involved. They are hyperemic if cut. Chronologically, this occurs during the stage of active tissue invasion following incubation. S. paratyphi may produce similar lesions in the stomach.146 During the lytic stage they develop areas of central necrosis corresponding to the microscopic mucosal necrosis and often are surrounded by a ring of hyperemia. The central pit intensifies with necrosis of the underlying lymphoid tissue, which releases bacterial toxins into the systemic circulation, causing intense clinical symptoms. Necrotic areas within the lymphoid tissue may coalesce (forming abscesses in some organs) and may slough (Fig. 19-6).
If the ulcer base includes a large blood vessel, it may bleed profusely; it is at this stage that transmural necrosis, usually of a Peyer’s patch, may result in perforation and peritonitis. Perforation usually occurs at the center of a Peyer’s patch in the terminal ileum close to the ileocecal valve on the antimesenteric border. Although these perforations are stated to be single, some series suggest that one-third of patients may have multiple perforations.147 On opening of the resected bowel, the enterocolitis is most apparent during this phase; the serosal surface of the gut is hyperemic and may have a fibrinous exudate. Mesenteric lymph nodes undergo similar changes, with yellow-gray areas of necrosis that may be confused with caseation. The colon is relatively uninvolved or normal.
Figure 19-6.Salmonella typhi.A: Disease involving the terminal ileum with large, pale areas expanding the submucosa. B: Detail shows these to be large, faintly eosinophilic macrophages (Mallory cells) mixed with other mononuclear cells, primarily lymphocytes. C: Gross specimen showing numerous round ulcers overlying lymphoid aggregates, some are quite deep and may perforate. (Courtesy of Dr. D. deSa.)
Histology During the invasive stage there may be a minimal increase in mononuclear cells of the lamina propria. Once tissue invasion has occurred, the lymphoid hyperplasia rapidly becomes apparent. This is manifested by an acute inflammatory infiltrate in the epithelium overlying lymphoid tissue (presumably in the M-cell region), although the underlying lymphoid tissue contains numerous macrophages that ingest cellular debris, neutrophils, and erythrocytes to form the characteristic typhoid (Mallory’s) cells (Fig. 19-6). This state may persist, forming a large inflammatory mass of histiocytes. In most instances, this progresses to necrosis and coalescence of adjacent necrotic foci, resulting in serpiginous, irregular zones of necrotic inflammatory cells in which histiocytes and neutrophils can still be identified. Because the lymphoid tissue usually remains submucosal, the underlying muscularis propria remains intact. However, larger Peyer’s patches may contain disease that involves the muscle layer. It is the end stage of this process involving the entire bowel wall that results in perforation. The mesenteric lymph nodes go through a similar series of changes.146
Campylobacter
Campylobacters are slender, spirally curved, motile, non-spore-forming gram-negative bacilli that are 0.5 to 4 µm in length.148, 149 The organisms are widespread in nature and may be found in a variety of animal feces, including domestic pets and cattle. There are about 16 species (e.g., fetus, jejuni, coli, faecalis, and sputorum) and several subspecies, of which 12 cause disease in humans.148Campylobacter is the most common stool isolate in the United Sates and developed countries and accounts for about 15% of patients with diarrhea.131 In many studies, it is the most frequent pathogen isolated and is more common than Salmonella, Shigella, Yersinia or Aeromonas.150, 151Campylobacters are transmitted by the fecal-oral route via contaminated water and food, and by direct contact with feces infected animals or humans. In the United States about 80% of cases are believed to be foodborne, and C. jejuni and C. coli account for over 95% of diagnosed cases.131 Most cases are sporadic, although small outbreaks occur from ingestion of raw milk or by swimming in, and presumably ingesting, contaminated water.152Campylobacter enterocolitis is also recognized as a sexually transmitted disease.48 The frequency of infection has only become apparent during the 1980s when the preferred growth conditions of the organism at 42°C were demonstrated. Campylobacter was originally thought to cause primarily an enteritis, but it is now apparent that colitis or proctitis is more common. The infection is seen throughout the year. In the United States and developed countries the peak incidence is in the summer and early fall, while in the developing countries and tropics there is no seasonal variation.149 It is also the commonest cause of diarrhea in travelers from developed nations.151 The infection is more common in immunocompromised patients, especially with HIV infection, and the disease tends to be more severe, chronic, and relapsing in these patients.
Pathogenesis. The organisms surviving the gastric milieu have the ability to penetrate and invade the small and large bowel epithelia, where they flourish and produce disease. The mechanisms of Campylobacter-induced disease are not clear, but two mechanisms have been postulated: (1) Intestinal adherence and toxin production and (2) Bacterial invasion and proliferation in lamina propria. Human isolates have been shown to produce toxin in vitro, as well as show adherence and invasive properties in cell culture studies.153 One of the toxins produced by the organism called cytolethal-distending toxin causes direct cell injury and arrests cells in G2M cell cycle.
Clinical and endoscopic features.C. jejuni is frequently associated with a gastroenteritis, which develops 1 to 7 days following ingestion of the organism.154, 155 The onset is abrupt, with flu-like symptoms, including fever and myalgias. Watery diarrhea with a frequency of 5 to 10 stools per day is the rule. Bloody diarrhea is common, often starting after about 3 days of disease. It is classically accompanied by lower abdominal colic and rectal bleeding on about the third or 4th day of infection, and in some patients abdominal pain is the predominant symptom and can be mistaken for acute abdomen. Some patients remain asymptomatic. Using molecular tests evidence of Campylobacter infection has been shown in about 19% patents with incidentally detected focal active colitis.156 The infection can spread to other parts of GI tract and can cause cholecystitis, pancreatitis, peritonitis, or rarely massive GI hemorrhage.149 Extraintestinal manifestations are rare and include septic arthritis, osteomyelitis, meningitis, endocarditis, and neonatal sepsis.157
The diagnosis is established with stool, and rarely blood cultures. The organisms can be identified by culture on selective media. Most microbiology laboratories are now equipped to identify the organisms, using special media and atmosphere. Selective cultivation at 42°C has dramatically improved the yield of C. jejuni from stool; on occasion the organism may only be cultured from rectal biopsy specimens but not from stoo1.158 Molecular methods of establishing the diagnosis are also available, however, they are seldom required in routine practice.
The disease is self-limited in most patients and resolves in 1 to 2 weeks, and requires only supportive treatment. Antibiotics are used for severe or prolonged cases, pregnant women and immunocompromised individuals.
Gross and endoscopic findings. Endoscopically, there is usually a proctocolitis with proximal infection in continuity for a variable distance, and mimicking ulcerative colitis when severe. Some patients have a focal and segmental disease that may include aphthoid ulcers and may therefore mimic Crohn’s disease.159, 160 In some, the colonoscopy may be unrevealing. Occasionally, inflammatory masses are described that may be mistaken for carcinoma.161, 162 Rare examples of massive hemorrhage that seem to originate from ulcers in the terminal ileum and ileocecal valve have been documented.163 Histology shows complete loss of mucosa at these sites. This may therefore be considered one of the rarest documented causes of “nonspecific” ulcers in this region.163
Histology. The histologic changes of C. jejuni infection are indistinguishable from any other forms of acute infectious colitis (Figs. 19-1 and 19-7).155, 164, 165 There is lamina propria inflammatory infiltrate rich in neutrophils with cryptitis and crypt abscesses. Inflammatory exudate, ulceration, and hemorrhage may be seen. Mild crypt distortion and loss can also be seen. In some cases with patchy inflammation Crohn’s disease, and in some cases with pan-colitis, ulcerative colitis enters the differential diagnosis. Conversely, some cases of IBD may present with superimposed Campylobacter infection (see later).
Figure 19-7.Campylobacter colitis. A: Overview of an otherwise classical acute infectious-type colitis, with reasonable architectural preservation and focal area of crypt loss that may occur in a severe case. B: A second patient with biopsy showing cryptitis, crypt abscesses, and lamina propria inflammation similar to any other case of acute infectious-type colitis. C: Higher magnification to show the cryptitis and crypt abscess formation. D: Severe Campylobacter colitis with what is virtually pus in the lamina propria; this is virtually diagnostic of acute infection.
Complications
Toxic Megacolon As in most other severe colitides, there are a few examples of fulminant disease, apparently from C. jejuni colitis, which have proceeded to toxic megacolon and have even required subtotal colectomy.166 Some patients have primarily proximal disease, most marked from the cecum to about the middescending colon, but relative distal sparing. We have also seen examples of fulminant enterocolitis in which the enteritis predominated and required resection (Figs. 19-8). Acute diverticulitis was also present.
Campylobacter Complicating Idiopathic Inflammatory Bowel Disease Patients with recurrent ulcerative colitis occasionally grow C. jejuni from their stool.53 The biopsy appearances that we have seen suggest that the underlying disease is indistinguishable from active ulcerative colitis and responds to local steroids. Under these circumstances, both steroids and antibiotics tend to be used. There is no evidence that antibodies to C. jejuni occur with more frequency in the colitic than in the noncolitic population.152
Figure 19-8. Fulminant Campylobacter enteritis in a patient with chronic lymphatic leukemia. (Courtesy of Dr. N. G. van der Westhuizen.) A: Resected small bowel with a thickened wall and a focally shaggy mucosa. B: Overview of mucosa, with ulcers on the left having deep fissures, as seen in any fulminant disease. C: Detail of fissuring, but also showing a band of serosal inflammatory cells. D: Detail shows mature lymphocytes, presumably a reflection of the patient’s underlying leukemia.
Other Complications One of the most important postinfectious complications is Guillain-Barré syndrome. Other rare postinfectious complications include HUS, uveitis, carditis, and encephalopathy.154, 167
Aeromonas hydrophila, Plesiomonas shigelloides, and Edwardsiella tarda
The list of organisms capable of causing diarrhea continues to grow and includes a variety of bacteria, including Plesiomonas shigelloides, Aeromonas species, and Edwardsiella tarda148, 149, 168, 169, 170, 171, 172, 173 (Table 19-1). The precise mechanism by which some of these organisms cause diarrhea is not clear, although a cholera-like toxin has been implicated in Plesiomonas.174, 175
Aeromonas are oxidase-positive facultatively anaerobic gram-negative bacilli. They are ubiquitous inhabitants of fresh and brackish water, and they have been even recovered from chlorinated water, including hospital water supply. They have been increasingly associated with diarrheal disease, apart from causing skin infection and sepsis. Infection is more common in children or individuals with underlying chronic illness or immunosuppression. They are particularly likely to cause diarrhea in children, and in one Australian study accounted for 10% of childhood diarrhea.176 In London, it accounted for 4.2% of isolates in patients with diarrhea, but in only one-half of these was there a possible symptomatic relationship.177 In some locales, they have been isolated as commonly as Shigella species or Campylobacter species. The carrier rate for this organism exceeds 25% in some parts of Asia. Among various species A. caviae, A. hydrophila, and A. sorbia are commonly isolated from diarrheal stools, and the predominant species varies depending on geographic location. The incidence of GI infection is highest in the late spring, summer, and early fall.
The diarrhea is most often mild and self-limited and antibiotics are required only with severe infection or septicemia. Some may develop nausea, vomiting, cramping, and abdominal pain. Some develop a subacute to chronic disease lasting from months to years mimicking IBD. About 15% to 25% of patients develop dysentery-like illness with blood, mucus, and fecal leukocytes, which may also mimic IBD endoscopically.
Plesiomonas shigelloides (formerly known as Aeromonas shigelloides) is a similar organism, which is oxidase-positive, facultatively anaerobic, and motile gram-negative bacillus. It is a ubiquitous fresh water inhabitant and has been implicated as a cause of acute diarrhea in adults and rarely also results in serious extraintestinal disease. It has been isolated from diarrheal stool from tropical and subtropical regions of Africa, Asia, and Australia. In the United States and Europe, it is seen in patients who traveled to tropical counties or with consumption of oysters or shellfish. It has also been implicated in diarrhea in travelers returning from Mexico or Caribbean. Apart from watery diarrhea, the symptoms may include cramping, abdominal pain, fever, headache, and vomiting. Some may present with dysentery with blood and mucus in the stool. The diarrhea is self-limited and antibiotics are not required.
Edwardsiella is frequently found in the stools of numerous animals, primarily reptiles, and with appropriate exposure appears to cause enteritis, which in one patient affected the terminal ileum and colon and was interpreted as Crohn’s disease.169 The organisms are oxidase-negative nitrate-positive gram-negative bacilli. Frequency of isolation from stools in individuals varies with geographic location, and many are asymptomatic.
Pathology. The gross and endoscopic features include mucosal edema, friability, exudates, and erosion or ulcers. The distribution is segmental and sometimes can mimic ischemic colitis or IBD. Rarely pancolitis may occur mimicking ulcerative colitis. The pathologic changes are similar and resemble any other self-limited colitis with neutrophilic-predominant lamina propria infiltrate, cryptitis, and crypt abscesses. Some degree of crypt distortion can be seen, which can mimic IBD. Even with crypt distortion all the changes in the crypt epithelium appear acute and of similar duration. Also, the basal plasmacytosis and crypt shortening of IBD are typically lacking.
Specific diagnosis of the infection is based on isolation of the organisms from stools and special efforts are required to identify them.
Legionella
There is a suggestion that Legionella pneumonia can be associated with exacerbations of preexisting IBD such as ulcerative colitis, with myriad organisms in the submucosa and a dramatic response to erythromycin.56
Yersinia Infection
Yersinia, like E. coli, belong to the Enterobacteriaceae, and are therefore gram-negative rods. Yersinia infection has a worldwide distribution and remains a common cause of bacterial enteritis. It is increasingly recognized as a pathogen, likely due to improved detection methods and has possibly resulted in a perceived increase in incidence. Currently there are eight species of Yersinia, but only three regularly affect humans. One of these is Y. pestis, which causes bubonic plague; the other two are Y. pseudotuberculosis and Y. enterocolitica. Both may be associated with acute terminal ileitis and mesenteric adenitis, although Y. enterocolitica is much more frequently associated with gastroenteritis. Y. pseudotuberculosis infections always appear to be with the same biogroup (biovar), although several serotypes have been identified. In contrast, Y. enterocolitica has five distinct biovars, depending largely on their fermentation characteristics and numerous serotypes; the latter, like Salmonella, are also characterized by their O and H antigens. The most frequently detected serotypes are 0:3 and 0:9 in Europe, 0:3 in Japan and Canada, and 0:8 in the United States. There is a marked regional variation in the frequency of isolation of Y. enterocolitica in patients with gastroenteritis. This is evident in North America, where isolation is much more frequent in Canada compared to much of the United States. There are rare reports of other Yersinia species causing gastroenteritis, including Y. frederiksenii and Y. kristensenii.178, 179Yersinia are also notable for producing a variety of secondary immune-mediated complications such as erythema nodosum, arthritis, and, infrequently, glomerulonephritis and Reiter’s syndrome.
Yersinia is widespread in nature but humans are likely the natural reservoir, particularly for Y. enterocolitica. Yersinia infection is transmitted by food and water, although person-to-person spread within families or in hospitals has also been documented. Infection can also be transmitted from animals. There are many animal reservoirs.180 The food products commonly associated with transmission of the infection include meat, poultry, dairy products, chocolate, and produce. Confirmed outbreaks of yersinial enteritis are uncommon and the means of infection are even less well documented, but they are often associated with milk. One outbreak in New York State was clearly related to infected chocolate milk181; in a second similar outbreak, powdered milk appeared to be the likely culprit.182 A multistate outbreak in the United States affecting thousands of people appeared to be the result of contamination of milk following pasteurization.183
Y. pseudotuberculosis is invariably pathogenic, but Y. enterocolitica is not. Since Yersinia grows preferentially at low temperatures, refrigerated food could be a source of infection, and it has also been suggested that infections are more common in cooler months.
Pathogenesis and clinical features. Specific serotypes of Y. enterocolitica and all Y. pseudotuberculosis are able to penetrate the epithelium and reach the adjacent lymph nodes, in which they may proliferate. The earliest ulcers in the terminal ileum are invariably over the domes of lymphoid follicles, an area where M-cells are known to predominate.184 Many Yersinia strains may produce toxins, but the role of toxins in causing disease has not been established. Y. pseudotuberculosis can produce an exotoxin; toxin-producing strains appear to be more virulent than non-toxin-producing strains.185Y. enterocolitica produces a heat-stable toxin, but not when incubated at more than 30°C, suggesting that preformed toxin may be important in outbreaks.185 Virulence in Yersinia appears to be mediated by plasmids, loss of which returns the organism to a nonvirulent strain.185 The growth and virulence of Yersinia are dependent on iron and stimulated by siderophores such as deferoxamine.
Yersinia lacks a natural high-affinity iron chelator; it cannot therefore absorb iron directly, but depends on iron attached to other bacterial siderophores in the gut for which it does have high-affinity receptors. Deferoxamine is a bacterial siderophore; developing Yersinia therefore has access to abundant siderophores in patients receiving the drug. Iron may also be plentiful if the patient is also being transfused for a congenital or acquired anemia or receiving hemodialysis. The median lethal dose of Yersinia in mice is reduced by a factor of 10 by iron dextran and 100,000-fold by deferoxamine.186 Patients receiving deferoxamine are therefore particularly likely to develop highly virulent Yersinia infections, peritonitis, hepatic abscesses, and other systemic complications.187 Because deferoxamine is almost completely eliminated in 30 hours, patients developing abdominal symptoms that may be attributable to Yersinia should consider temporarily stopping deferoxamine.187 There have been several reports of patients developing Yersinia infection following hemodialysis.188, 189
Yersinia infection has been associated with enterocolitis, terminal ileitis (pseudoappendicitis syndrome), and appendicitis. Y. enterocolitica affects both sexes, primarily in the first two decades of life. It may produce either a severe terminal ileitis associated with hemorrhagic necrosis of the mucosa or a gastroenteritis clinically indistinguishable from that produced by other enteric pathogens. Also, because the gastroenteritis associated with Y. enterocolitica may be self-limited and not associated with any structural changes, it is possible that in some cases isolation of the organism may represent an incidental finding. Many patients harboring the organism appear to have relatively few symptoms.179 Before Yersinia was easily cultured, some cases were almost certainly described as “acute terminal ileitis (pseudoappendicitis syndrome).” Although this rare condition was first presented in the original classical description of Crohn’s disease, it is also the most frequent clinical manifestation of Yersinia infection and clinically mimics acute appendicitis, sometimes with a generalized lymphadenopathy. The identification of Yersinia as the etiology of acute terminal ileitis provided an easy explanation of why the disease resolved spontaneously in many patients and did not progress to overt Crohn’s disease. It is now estimated that 50% to 80% of all acute terminal ileitis is Yersinia associated.190, 191 The diagnosis is made by culture of stool or appendiceal swab if resection has been carried out. In addition, seroconversion with a marked rise in titer 2 to 3 weeks following infection confirms the diagnosis. It should be added that if laparotomy is carried out the appendix should usually be removed, for even if the underlying disease is Crohn’s disease, there is no additional risk of cutaneous fistulas (see Chapter 18).
Yersinia pseudotuberculosis infection predominantly affects 5- to 15-year-old males, with about a 5:1 male:female ratio.192 It produces symptoms that may be indistinguishable from those of acute appendicitis; the presence of cervical adenopathy is a pointer to the underlying pathology. If laparotomy is carried out, mesenteric adenitis is invariably found, with or without terminal ileal disease and usually with only mild appendiceal inflammation. An interesting study of patients with high concentrations of yersinial antibodies found that some patients with specific subtypes of antibodies to both Y. enterocolitica serotype 9 and Y. pseudotuberculosis 1A had a genuine appendicitis; two with antibodies against serotype 3 had terminal ileitis or mesenteric adenitis; and, surprisingly, four had pancreatitis, two associated with cholecystitis.193
Most infections are generally self-limited and there is no evidence that antibiotics alter the natural course of infection, and may even predispose to it.179 They are used mainly when there is evidence of septicemia. Septicemia is rare and tends to occur in immunosuppressed individuals or those with hemolytic anemias; however, the mortality is about 50% despite therapy.185
There is marked variability in the proportion of patients developing chronic disease, being only 0% to 4% in many series, with an average of 1%.194 In Sweden, however, the figure is considerably higher; overall, about 14% of patients go on to develop chronic terminal ileitis that mimics Crohn’s disease; however, in this situation the other possibilities are that the organism was an incidental finding in a patient with Crohn’s disease, or that the infection unmasked underlying Crohn’s disease.
Gross pathology and endoscopic appearances. Lymph nodes are markedly enlarged and may reach 4 cm in size. On section, yellow-gray foci of necrosis may be apparent. When appendix is involved it may appear a little injected or diffusely thickened or may be the seat of periappendicitis. Terminal ileal involvement causes a thickened, edematous bowel wall. Lymphoid tissue may bulge into the lumen, and mucosal hemorrhages may be present.
Smaller aphthoid ulcers may be seen diffusely scattered throughout the involved bowel, and in some cases be in continuity with terminal ileal disease195; the intervening mucosa may appear surprisingly normal.196, 197 Endoscopically, punctate aphthoid ulcers may be localized to the rectosigmoid or may occur focally elsewhere in the colon; they may also be seen in ileostomy sites.195 In some patients, diffuse inflammation mimicking ulcerative colitis may be seen, with friability and loss of vascular pattern. It is also apparent that some patients with ulcerative colitis may grow Yersinia but respond to conventional therapy for ulcerative colitis.179
With Yersinia enterocolitis terminal ileal involvement is invariably seen, which may extend well into the colon; surprisingly, the appendix may be uninvolved. The bowel wall is focally thickened and nodular and may form inflammatory polypoid masses (Fig. 19-9); one of the masses is usually dominant, and smaller nodules may be present. The adjacent mucosa has numerous aphthoid ulcers that tend to diminish in intensity proximal and distal to the ileocecal valve. Ulcers can be seen, which tend to be longitudinal and are largest in the terminal ileum. They may reach a size of 5 cm or more, and may extend into the large bowel as smaller lesions. Perforation occurs rarely, primarily in debilitated patients or those taking deferoxamine (Fig. 19-10). The remaining mucosa may be hyperemic or surprisingly normal. The serosa may have a slight exudate and rarely peritonitis may occur. The classical syndrome is one in which mesenteric lymph nodes are enlarged but usually lack evidence of necrosis on the cut surface unless fulminant or perforating disease is present.
It has also become increasingly apparent that Y. enterocolitica can cause a self-limited colitis resembling Crohn’s disease and sometimes ulcerative colitis; it is relatively common and in one study accounted for 10% of stools containing pathogens.179
Histology.Y. enterocolitica: In resections, which are invariably of the terminal ileum, Y. enterocolitica produces a characteristic microscopic appearance. Sections taken of the smallest aphthoid ulcers or even red spots in the ileum show a lymphoid nodule with ulceration of the dome epithelium (M-cells), which is replaced by zoned necrosis consisting of a fibrinopurulent exudate in which neutrophils are usually present (Fig. 19-9D). Beneath the exudate there may be a zone of necrotic debris, in or beneath which organisms can often be found. Beneath this is a zone of histiocytes that tend to palisade focally, and beyond this is the remainder of the preexisting lymphoid nodule, which may be no larger than those usually seen in the terminal ileum. Larger inflammatory masses recapitulate this theme on a grander scale. They consist of hyperplastic lymphoid tissues that expand the submucosa and at the center of which the same zoned necrosis is seen (Fig. 19-9D). This usually resembles vertical fissures, although these do not usually penetrate further than the level of the original submucosa. Although the palisaded histiocytes are well demarcated, they do not form the well-circumscribed granulomas of Y. pseudotuberculosis (see later) or Crohn’s disease. Adjacent mucosa may show a range of changes from edema to acute and chronic inflammation, and like many infections tends to be crypt sparing. The submucosa is very edematous and frequently contains a diffuse neutrophilic infiltrate reminiscent of a phlegmon. In fulminant disease this multilayered inflammatory infiltrate may be much less characteristic, retaining the neutrophils and necroses but losing the zone of histiocytes (Fig. 19-10). Lymph nodes tend to show reactive changes only,198 but occasionally, and particularly in fulminant disease, the same zoned necrosis may be present in an irregular stellate fashion, but not in the well-demarcated manner of Y. pseudotuberculosis.195, 196
Figure 19-9.Yersinia enterocolitica terminal ileitis. A: Gross photograph showing the large inflammatory nodules together with minute white pinpoint nodules of lymphoid tissue, many of which are also involved. B: Section through a larger nodule with fissuring ulceration; despite the size of the nodules grossly, the inflammation is limited almost entirely to the submucosa. C: Detail illustrates the superficial, partially necrotic zone, in which neutrophils predominate, and the underlying zone of histiocytes. D: Section of barely visible lymphoid nodule showing the early lesion developing on the surface of the epithelium and involving the superficial part of the nodule itself. (Courtesy of Dr. R. Rickert.)
Figure 19-10. Fulminant Yersinia with perforation in a patient taking deferoxamine and being transfused. A: Gross specimen showing edematous, diffusely ulcerating disease, which in the mesenteric border of the ileum can be seen to extend through the muscle and into the adjacent necrotic lymph nodes and mesenteric fat. The antimesenteric border of the ileum is the site of perforation (arrow). Hepatic abscesses were also present. B: Section at the perforation site showing fissuring ulceration (left) and perforation (upper right). C: Detail of the fissures showing necrosis in the wall but lack of the zoning effect seen in Figure 19-9. D: The relatively unaffected adjacent small and large bowels have marked submucosal edema and inflammation, suggesting local phlegmonous enterocolitis.
The biopsy appearance in infective yersinial colitis is not well documented but seems to consist of focal neutrophils, primarily at the edges of ulcers, and epithelioid histiocytes—a combination that replicates changes found in resection. Plasma cells are inconspicuous, and no giant cells or well-formed granulomas are found.195
Yersinia pseudotuberculosisinfection. The characteristic lesion of Y. pseudotuberculosis consists of multiple necrotizing granulomas with stellate central necrosis and a mass of neutrophils surrounded by histiocytes at the periphery. These changes are essentially indistinguishable from those found in lymphogranuloma inguinale or cat-scratch disease; however, these diseases are extremely uncommon in mesenteric nodes, rarely cause intestinal mucosal disease, and, given their completely different clinical histories, should not pose a diagnostic problem. These necrotizing granulomas are frequently multiple. Nodes may also have capsular thickening, a polymorphous inflammatory infiltrate, and follicular hyperplasia, often with a histiocytic proliferation in the interfollicular region, which seems to be the earliest manifestation of the disease. Necrotizing granulomas or granulomas without necrosis may also occur (Fig. 19-11), and some nodes may contain no granulomas.198
Figure 19-11.Yersinia infection of the terminal ileum. A: A background of lymphoid hyperplasia with scattered epithelioid cell granulomas. B: Closer look at the granulomas in this case shows histiocytes with deep eosinophilic granular cytoplasm similar to those seen with Malakoplakia, with which it has been associated is some cases. C:Yersinia infection of the rectum showing similar findings with a background of lymphoid hyperplasia with scattered epithelioid cell granulomas. D: Closer look at the granulomas in this case show histiocytes with deep eosinophilic granular cytoplasm.
Only gold members can continue reading. Log In or Register to continue