Embryonal Tumor with Abundant Neuropil and True Rosettes
Peter C. Burger, MD
Key Facts
Terminology
Relationship to ependymoblastoma debated
Clinical Issues
Usually < 3 years
Intracranial, both supra- and infratentorial
Poor prognosis; highly aggressive
Image Findings
Large
Well circumscribed
Little if any contrast enhancement
Microscopic Pathology
Highly cellular unstructured primitive areas
Paucicellular finely fibrillar neuropil
True rosettes
Focal differentiation, in neuropil areas, to neurocytes and ganglion cells in some cases
Rosette lumina delineated by zone composed of cell-cell junctions
Features of anaplasia similar to anaplastic medulloblastoma in some cases
Ancillary Tests
Synaptophysin(+), especially neuropil areas
Amplification 19q13.42
Diagnostic Checklist
Abundant neuropil highly suggestive of entity
Rosettes may be inconspicuous
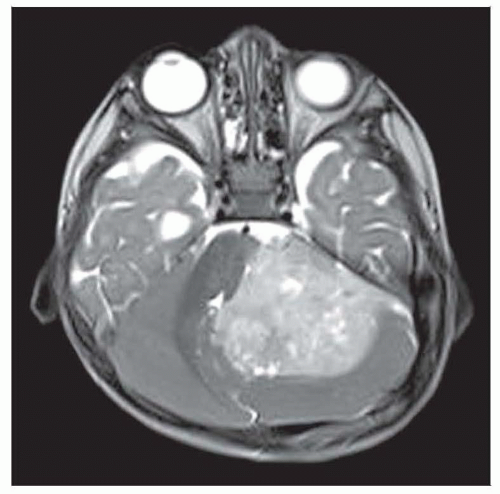 As in this T2WI of a cerebellar example, the lesion is often well circumscribed. There is typically little enhancement. |
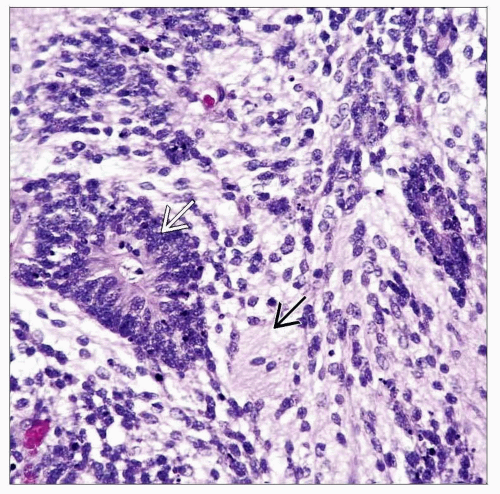 Distinctively, the tumor combines finely fibrillar neuropil  and true, lumen-containing rosettes and true, lumen-containing rosettes  . . |
TERMINOLOGY
Abbreviations
Embryonal tumor with abundant neuropil and true rosettes (ETANTR)
Synonyms
Neuroblastic tumor with abundant neuropil and true rosettes
Embryonal tumor with abundant neuropil and ependymoblastic rosettes
Definitions
Embryonal tumor formed of finely fibrillar neuropil and lumen-containing, true rosettes
Relationship to ependymoblastoma debated
ETANTR closely related or equivalent to ependymoblastoma, or
Ependymoblastoma is unrelated to ETANTR
CLINICAL ISSUES
Epidemiology
Age
Usually < 3 years
Gender
F > M
Site
Intracranial, both supra- and infratentorial
Presentation
Signs of increased intracranial pressure
Treatment
Surgical approaches
Resection
Adjuvant therapy
Chemotherapy
Radiation
In some cases, despite patient age
Prognosis
Poor, highly aggressive
Most die within 36 months
Median survival: About 9 months
Potential for CSF seeding
IMAGE FINDINGS
MR Findings
Large, well circumscribed
Little if any contrast enhancement in most cases
MACROSCOPIC FEATURES
General Features
Fleshy, reddish-gray



