Embryonal Carcinoma
Key Facts
Terminology
Embryonal carcinoma adult type
Clinical Issues
Incidence
Unusual tumor in its pure form
More often accompanied with another germ cell tumor, mainly yolk sac tumor
May account for no more than 10% of all mediastinal germ cell tumors
More common in young adults; unusual in older individuals
More common in 3rd decade of life
More common in males
Symptoms
Chest pain
Cough
Dyspnea
Klinefelter syndrome
Hematologic dyscrasias
Chromosomal abnormalities
Microscopic Pathology
Gland-like appearance
Sheets of neoplastic cells
Primitive cellular proliferation
Cells with prominent nucleoli
Extensive necrosis
Prominent cellular atypia and mitotic activity
Top Differential Diagnoses
Anaplastic large cell lymphoma
Metastatic adenocarcinoma of lung origin
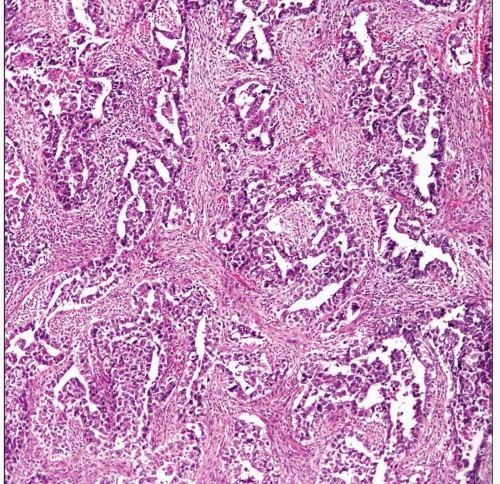 Embryonal carcinoma shows the typical glandular arrangement of neoplastic cells separated by inflamed fibroconnective tissue. |
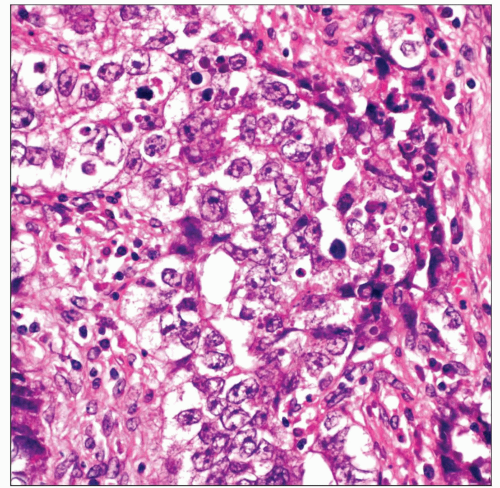 Closer view of the neoplastic cells shows medium-sized cells with round to oval vesiculated nuclei and prominent nucleoli. These features are typical of embryonal carcinoma. |
TERMINOLOGY
Abbreviations
Embryonal carcinoma (EC)
Synonyms
Embryonal carcinoma adult type
Definitions
Malignant germ cell tumor
ETIOLOGY/PATHOGENESIS
Etiology
Although a definitive etiology is unknown, misplaced germ cells in mediastinum may be the origin of these tumors
CLINICAL ISSUES
Epidemiology
Incidence
Unusual tumor in its pure form
More often accompanied with another germ cell tumor, mainly yolk sac tumor
May account for no more than 10% of all germ cell tumors of mediastinum
Age
Tumor is more common in young adults
More common in 3rd decade of life
Unusual in older individuals
Gender
More common in males
Unusual cases in females have been described
Presentation
Chest pain
Cough
Dyspnea
Klinefelter syndrome
Hematologic dyscrasias
Chromosomal abnormalities
Treatment
Chemotherapy
Cis platinum-based therapy
Surgical debulking if appropriate
Prognosis
Poor
May depend on clinical staging
IMAGE FINDINGS
General Features
Anterior mediastinal tumor
Bulky tumor indistinguishable from other nonteratomatous germ cell tumors
MACROSCOPIC FEATURES
General Features
Large, ill-defined tumors
Extensive necrosis and hemorrhage
Sections to Be Submitted
Extensive sampling is required
Possible sites of involvement
Lung
Pericardium
Lymph nodes
Diaphragm
Size
Variable from a few cm to > 10 cm in diameter
MICROSCOPIC PATHOLOGY
Histologic Features
Gland-like appearance
Sheets of neoplastic cells
Primitive cellular proliferation
Cells with prominent nucleoli
Extensive necrosis
Prominent cellular atypia and mitotic activity
Predominant Pattern/Injury Type
Necrosis
Predominant Cell/Compartment Type
Germ, nonseminomatous
ANCILLARY TESTS
Electron Microscopy
Transmission
Intercellular junctions and desmosomes
Tight junctions and telolysosomes
DIFFERENTIAL DIAGNOSIS
Metastatic Adenocarcinoma of Lung Origin
Glands in adenocarcinoma are better formed
Glands in adenocarcinoma may show positive intracellular mucin
Adenocarcinoma of lung origin may show positive staining for TTF-1
Lung adenocarcinomas are more common in older patients unlike young age in EC
Would be highly unusual for lung adenocarcinoma to show positive staining for CD30
Seminoma
Seminomas show more cohesive growth pattern
Seminomas rarely show extensive areas of necrosis
EC may show positive staining for CD30 while negative in seminomas
EC shows more prominent nuclear atypia and mitotic activity
Yolk Sac Tumor
YST and EC may show similar histopathological pattern
YST and EC may show similar immunophenotype
Presence of prominent nucleoli in EC may help in separating these tumors
Mixed Germ Cell Tumor
Extensive sampling is of utmost importance
EC is often accompanied with another germ cell tumor, namely yolk sac tumor
Thymic Carcinoma
Some high-grade carcinomas of thymus may share some histopathological features
Thymic carcinoma does not show staining for α-fetoprotein or CD30
Anaplastic Large Cell Lymphoma
Anaplastic large cell lymphoma and EC may show positive staining for CD30 and EMA/MUC1
Does not show positive staining for α-fetoprotein
DIAGNOSTIC CHECKLIST
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


