Congenital Dyserythropoietic Anemia
Kathryn Foucar, MD
Key Facts
Terminology
Hereditary erythrocyte maturation disorder
Bone marrow required for diagnosis
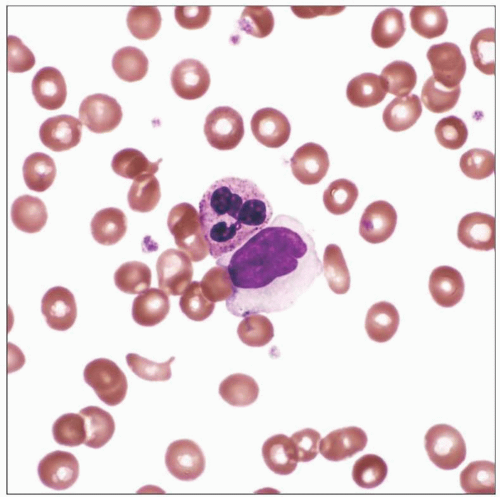
Distinctive morphologic abnormalities of erythroid cells, including internuclear bridging and multinucleation
3 major subtypes
Etiology/Pathogenesis
Autosomal recessive or autosomal dominant inheritance
Genetic defect in mitosis
Ineffective erythropoiesis
Reticulocyte count low for degree of anemia
Blood and bone marrow abnormalities present at birth, but patient may not manifest until middle age
Most cases diagnosed by early adulthood
Microscopic Pathology
Blood
Variable degree of anemia
Variably prominent anisopoikilocytosis
Bone marrow
Prominent erythroid hyperplasia
Variable megaloblastic changes, multinucleation, nuclear budding, karyorrhexis, and internuclear bridging
Other bone marrow lineages are unremarkable
Ancillary Tests
Genetic testing for CDAN1 mutations
Defects in nuclear membrane prevalent by EM
Cytoplasmic contents may spill through nuclear membrane defects into nucleus by EM
 Peripheral blood smear from a 60-year-old woman with CDA III shows anemia, macrocytosis, and mild anisopoikilocytosis. (Courtesy R. Brynes, MD.) |
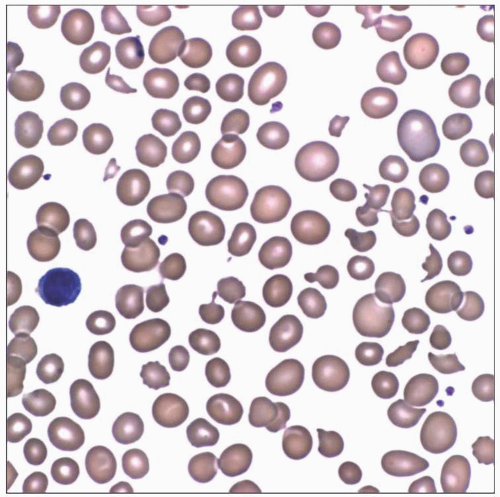 Peripheral blood smear from a 39-year-old woman with longstanding macrocytic anemia shows marked anisopoikilocytosis; blood and bone marrow are compatible with CDA II. |
TERMINOLOGY
Abbreviations
Congenital dyserythropoietic anemia (CDA) I-III
Synonyms
Hereditary erythroblast multinuclearity with positive acidified serum (HEMPAS) (for CDA II)
Definitions
Hereditary erythrocyte maturation disorder
Variably severe anemia
Anisopoikilocytosis of red blood cells (RBC)
Distinctive morphologic abnormalities of erythroid lineage cells within bone marrow
Internuclear bridging
Multinucleation
Nuclear budding, karyorrhexis
3 major subtypes
ETIOLOGY/PATHOGENESIS
Genetic Features
Autosomal recessive or autosomal dominant inheritance
Genetic defect primarily involving mitosis
Genetic localization for CDA I, II, III described
CDAN1 mutation in CDA I results in abnormal codanin-1 protein
Pathogenesis
Ineffective erythropoiesis
Increased erythroid lineage in bone marrow with inadequate erythrocyte production
Reduced reticulocyte count for degree of anemia
Incidence/Ethnicity
Rare; generally limited to family kindreds or geographic regions
Italy, Sweden, Israeli Bedouins, Lebanon, India, Japan, China
Approximately 400 family kindreds in Europe
Some association with consanguinity for autosomal recessive types
Very rare sporadic cases
CLINICAL ISSUES
Presentation
Age
Blood & bone marrow abnormalities present at birth
Age at disease presentation highly variable
May manifest at birth or early infancy
Manifestation may be as late as middle age
Most cases diagnosed by early adulthood
May be asymptomatic
Symptoms of chronic moderate to severe anemia
Some patients may be jaundiced
Splenomegaly with variable hepatomegaly by adulthood in CDA I, CDA II
Some patients have skeletal abnormalities
Rare patients present with dysmorphic features
Laboratory Tests
Reticulocyte count suboptimal for degree of anemia
LDH (lactic dehydrogenase) elevated
Indirect bilirubin elevated in CDA I, CDA II
Acidified serum test positive in CDA II
RBC agglutination by anti-i & anti-I positive in CDA II
Variable in CDA I and CDA III
SDS-PAGE (polyacrylamide gel electrophoresis)
Abnormal in CDA II and CDA III
Genetic testing for codanin mutations may be positive
Treatment
Prognosis
Generally excellent
Iron overload adverse impact
IMAGE FINDINGS
Radiographic Findings
Skull and other bone lesions due to increased hematopoiesis
Mediastinal and paravertebral masses due to extramedullary hematopoiesis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


