Colon: Diagnosis and Margins
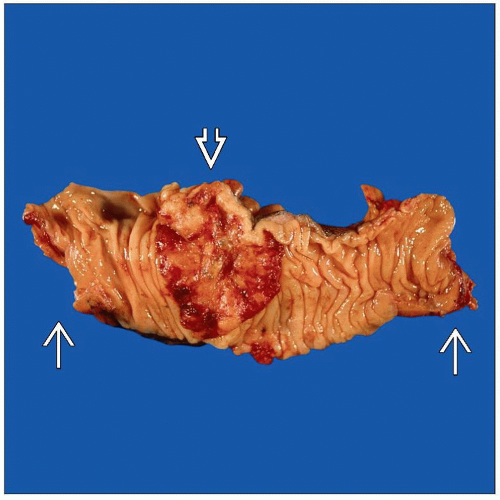 This invasive colon carcinoma  is located far from the proximal and distal margins is located far from the proximal and distal margins  . Frozen section is unnecessary if the mucosa at the resection margins appears normal on gross examination. . Frozen section is unnecessary if the mucosa at the resection margins appears normal on gross examination. |
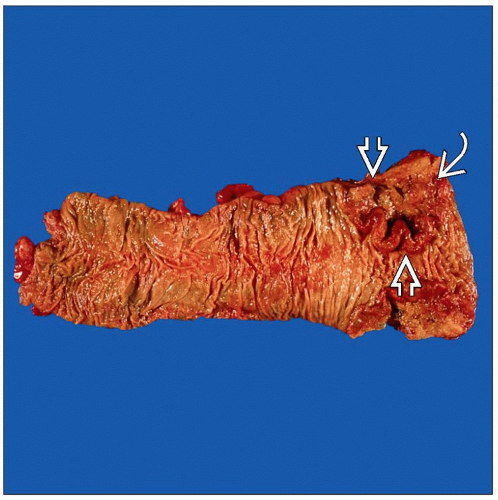 Rectal cancer  may be resected very close to the distal margin may be resected very close to the distal margin  to spare the sphincter muscles. Frozen section to accurately determine distance to margin is justified in these cases. to spare the sphincter muscles. Frozen section to accurately determine distance to margin is justified in these cases. |
SURGICAL/CLINICAL CONSIDERATIONS
Goals of Consultation
Verify that lesion is present in resected colonic segment
Evaluate margins
Measure length of uninvolved colon to distal margin in low rectal resections
Change in Patient Management
If a margin is involved by tumor, additional colon may be resected
Clinical Setting
Some colonic lesions may be difficult to detect intraoperatively by palpation
Polyps previously biopsied and shown to have small areas of carcinoma
Carcinomas after neoadjuvant therapy
Surgeons often request colon be opened and returned to operating room
Length of uninvolved colon to distal margin for rectal lesions may be used in deciding on value of radiation therapy
SPECIMEN EVALUATION
Gross
Identify colon segment according to structures present
Right colectomy: Terminal ileum, cecum, appendix, ascending colon
Transverse colon: Colon with mesentery
Sigmoid colon: Colon with mesentery
Low sigmoid/rectum: Mesentery on proximal portion; distal portion lacks mesentery and serosa
Identify location of any lesions as being in sigmoid, at sigmoid/rectal junction, or in rectum
If carcinoma is close to distal margin, specimen is likely distal sigmoid/rectum
Anterior/posterior resection: Sigmoid, rectum, and anus
Examine outer surface and identify following if present
Gross involvement by carcinoma
Perforation may be associated with inflammatory changes
Puckering of serosa in area of intracolonic mass
Usually indicates carcinoma has invaded visceral peritoneum
Metastatic lesions to serosa
May be associated with inflammation, causing bowel segments to be adherent
Tattoo ink may be present, marking site of prior polypectomy
Palpate specimen to identify site of intraluminal lesion and any grossly involved lymph nodes
Open colon along antimesenteric side with blunttipped scissors, avoiding transecting any lesions
Cut open stapled margins completely, as close to staple line as possible
If necessary, mucosa can be gently rinsed clean with saline
Tap water is hypotonic and may damage tissue
Identify all lesions and relationship to margins
Bowel segments can contract up to 40% within 10-20 minutes after excision
Measure and record distances to margins
Most important for distal margin for rectal cancers
If no lesion is apparent, contact surgeon
If lesion was a polyp that was previously biopsied, site of polyp may be subtle area of mucosal ulceration
Biopsy site may be in area of tattoo ink
If surgeon wishes to view specimen in operating room, specimen should be transferred to clean surgical drape or pad
Specimen must be placed in appropriately labeled container for transfer
Frozen Section
May be useful for margin evaluation in the following cases
Prior treatment, making extent of tumor difficult to evaluate grossly
Carcinoma arising in background of inflammatory bowel disease, making margin evaluation difficult
Signet ring cell carcinomas
Infiltrative pattern in submucosa and muscularis can occur
Mucosal surface is often normal in appearance
If grossly evident carcinoma is present near margin, margin can be taken as perpendicular section
If grossly evident carcinoma is not seen, but diffusely invasive carcinoma is known or suspected, en face section will show larger area of margin
MOST COMMON DIAGNOSES
Adenocarcinoma
Colon carcinomas are generally easily recognizable as a raised tan/brown mass arising from mucosa
Central ulcerated center or circumferential growth pattern are typical
Cut surface is firm and homogeneously white
Invasive carcinoma effaces normal muscularis propria and may penetrate into pericolonic adipose tissue
Typical carcinoma has tall columnar cells forming tubules, complex cribriform proliferations, or solid nests
Extensive dirty necrosis is common
Less common histologic types are mucinous, medullary, and signet ring cell
Carcinoma does not extend microscopically beyond grossly recognizable mass
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


