Collecting Duct Carcinoma
Satish K. Tickoo, MD
Victor E. Reuter, MD
Key Facts
Terminology
Collecting duct carcinoma (CDC)
Rare, high-grade renal cell carcinoma likely arising from cells of collecting ducts of renal medulla
Diagnostic features still evolving, with characteristic but not entirely specific, morphologic and immunophenotypic features
Collecting duct carcinoma (CDC)
Clinical Issues
Occurs over wide range (13-83 years) but mostly in patients 50 or younger
Predominantly centered in medulla of kidney
1/2 of patients dead of disease within 2 years
Microscopic Pathology
Primarily high-grade adenocarcinoma
Variable architectural patterns, usually in various combinations, including tubular, papillary, solid, cribriform
Typically with multinodular growth pattern, desmoplastic stroma, and intratumoral inflammatory infiltrate
Ancillary Tests
Often stain positive with lectins, ULEX-1, PNA, and soybean agglutinin
Top Differential Diagnoses
Papillary renal cell carcinoma
Urothelial carcinoma with glandular features
Metastatic carcinoma
Other tumors, including renal medullary carcinoma and HLRCC syndrome tumors
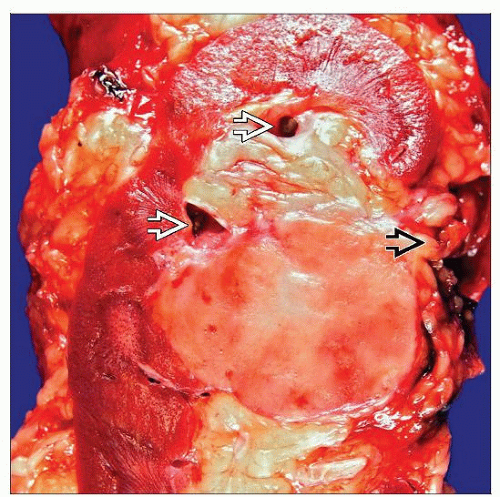 This example of CDC centered in the renal medullary region of a kidney shows a somewhat homogeneous cut surface. Extension into sinus fat  and pelvicalyceal system and pelvicalyceal system  are common. are common. |
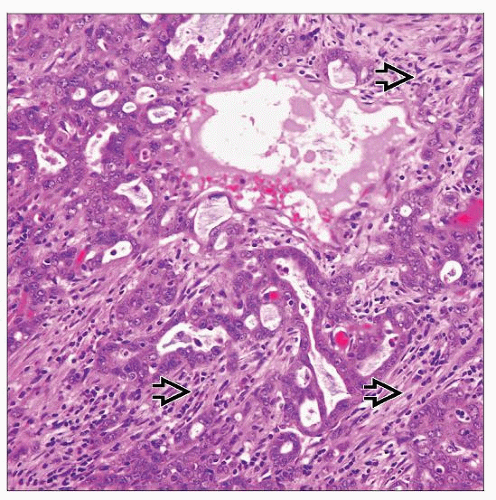 Microscopically, collecting duct carcinoma is a high-grade adenocarcinoma that may show variable architectural patterns. Multinodularity and abundant stromal desmoplasia  are characteristic. are characteristic. |
TERMINOLOGY
Abbreviations
Collecting duct carcinoma (CDC)
Synonyms
Carcinoma of collecting ducts of Bellini
Definitions
Rare, high-grade renal cell carcinoma, likely arising from cells of collecting ducts of renal medulla
Diagnostic features still evolving, with characteristic but not entirely specific morphologic and immunophenotypic features
ETIOLOGY/PATHOGENESIS
Genetic Features
Monosomies of chromosomes 1, 6, 14, 15, and 22 consistently observed in the few tumors tested
Loss of heterozygosity (LOH) of multiple chromosomal arms, including 1q, 6p, 8p, 13q, and 21q present in most cases
Minimal area of deletion located at 1q32.1-32.2 also identified
Amplification of HER2 present in some cases
Trisomies of 7 and 17 (typical of papillary RCC) are absent
Chromosome 3 losses (typical of clear cell RCC) not present
CLINICAL ISSUES
Epidemiology
Incidence
Constitute < 1% of malignant renal cell tumors
Until recently, largest series in literature included a mere 12 cases
Recent nationwide survey study from Japan was able to include 81 cases in their report
Age
Occurs over wide range of 13-83 years
Mean age is close to 50 years in different studies
Site
Predominantly centered in medulla of kidney
In larger tumors, site of origin difficult to determine
Presentation
Hematuria
Palpable flank mass, pain, and weight loss
Symptoms related to metastases
Unlike what is usual in more common RCC subtypes, approximately 2/3 cases symptomatic at presentation
Treatment
Currently, surgical excision and urothelial carcinoma-like chemotherapeutic options commonly followed
Responses to any therapy very limited and of short duration
Recently, targeted therapies against tyrosine kinase receptors of VEGF-related molecules have shown some promise
Prognosis
Unfavorable outcomes very common
Approximately 1/2 of patients die of disease within 2 years
Frequently metastatic at presentation, commonly with multiple organ involvement, including
Lymph nodes (44%)
Various viscera (32%), with lungs being most common site (17%)
Bones (16%) with both osteolytic and osteoblastic lesions
MACROSCOPIC FEATURES
General Features
Predominantly located in medulla, but larger tumors often involve cortex secondarily
Classically, gray-pale with invasive borders
Typically has multinodular growth pattern
Areas of necrosis, hemorrhage, and cystic change are frequently present
Grossly, majority of tumors invade renal sinus and perinephric fat
Well-circumscribed tumors with purely cystic appearance previously considered low-grade CDC
Currently, such tumors regarded as separate entity, “tubulocystic carcinoma”
Whether these represent distinct tumor entities or variations in morphologic spectrum of CDC is not clear at present
Some CDCs with otherwise typical high-grade features also show variable amount of tubulocystic areas
Size
1-15 cm (median: 6 cm)
MICROSCOPIC PATHOLOGY
Key Descriptors
Predominant Pattern/Injury Type
Neoplastic
Predominant Cell/Compartment Type
Epithelial
Histologic Features
Primarily high-grade adenocarcinoma
Variable architectural patterns, usually in various combinations
Including tubular, solid tubular/acinar, papillary, solid sheet-like, cribriform, and (rarely) diffuse signet ring cell-like
Like other RCCs, CDCs may also show sarcomatoid features
Biologic significance of such features not as dramatic as in other RCCs, as usual CDC by itself is very aggressive tumor
Multinodular growth pattern with marked desmoplastic stroma and intratumoral inflammatory infiltrate, including microabscesses
Surrounding renal collecting ducts often show dysplastic cytologic features
High-grade cytology, often with marked nuclear pleomorphism and brisk mitotic activity
Sometimes cytoplasmic mucin may be seen, highlighted by Alcian blue or mucicarmine stain
Lymphatic/Vascular Invasion
Present in majority of cases
Lymph Nodes
Metastases to regional nodes frequent in CDC
ANCILLARY TESTS
Immunohistochemistry
Generally positive for
HMCK(34βE12), EMA/MUC1, CK7, CEA
Often stain positive with lectins, ULEX-1, PNA, and soybean agglutinin
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


