Chromophobe Renal Cell Carcinoma
Satish K. Tickoo, MD
Victor E. Reuter, MD
Key Facts
Terminology
Chromophobe renal cell carcinoma (Ch-RCC)
Characterized by large pale and smaller eosinophilic tumor cells in variable proportions, with wrinkled nuclei and perinuclear halos
Etiology/Pathogenesis
Ch-RCC typically shows combined chromosomal losses usually affecting chromosomes 1, 6, 10, 13, 17, 21, and Y
Clinical Issues
Prognosis of Ch-CRC much better than clear cell RCC, and also than papillary RCC in some studies
Sarcomatoid features in tumor; most frequent association with aggressive clinical behavior
Microscopic Pathology
Pattern of growth is predominantly solid, separated by thin, incomplete fibrovascular septa
In “classic” type tumors, predominant cell type is that with a pale, somewhat clear-appearing cytoplasm
In “eosinophilic” variants, predominance of tumor cells with densely eosinophilic, granular cytoplasm
Most tumors show admixture of pale and eosinophilic cells
Most characteristic histological feature: Hyperchromatic nuclei with irregular, wrinkled outlines (“raisinoid” nuclei)
Another characteristic feature: Presence of perinuclear cytoplasmic clarity (perinuclear halos)
Presence of cytoplasmic microvesicles is unique and consistent ultrastructural feature of Ch-RCC
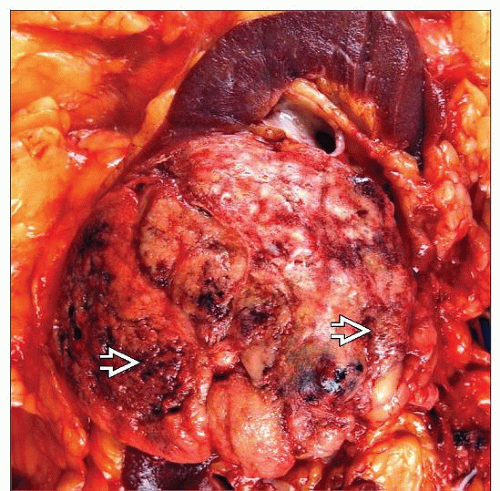 Chromophobe renal cell carcinoma is typically well circumscribed, with tan-gray, multilobulated cut surface. Hemorrhage and necrosis  are grossly identified in more than a quarter of the cases. are grossly identified in more than a quarter of the cases. |
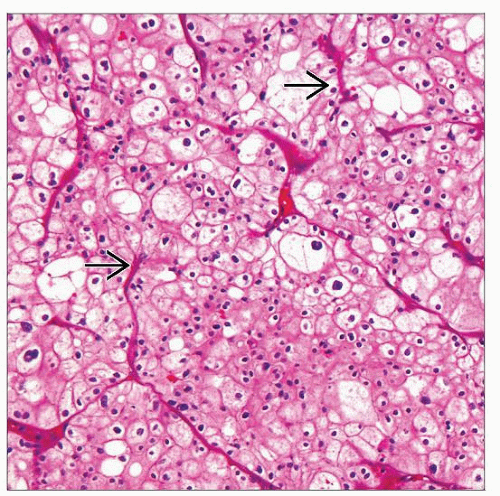 Typically, a chromophobe renal cell carcinoma shows solid sheets of clear and eosinophilic cells, separated by thin and incomplete  vascular septations that do not completely encircle cell nests. vascular septations that do not completely encircle cell nests. |
TERMINOLOGY
Abbreviations
Chromophobe renal cell carcinoma (Ch-RCC)
Definitions
3rd most common subtype of renal cell carcinoma
Characterized by large pale and smaller eosinophilic tumor cells in variable proportions, with wrinkled nuclei and perinuclear halos
ETIOLOGY/PATHOGENESIS
Genetic Features
Ch-RCC typically shows combined chromosomal losses usually affecting chromosomes 1, 6, 10, 13, 17, 21, and Y
Loss of multiple chromosomes leads to almost consistently present hypodiploidy
Abnormalities in mitochondrial DNA may be observed, but their specificity remains controversial
Recently, gene expression profiling has shown up-regulation of a number of genes encoding proteins integrated to membranes
Many of these up-regulated gene products are related to vesicle-mediated transport
Cell of Origin
Ch-RCC are thought to arise from intercalated cells of renal cortex, similar to renal oncocytomas
CLINICAL ISSUES
Epidemiology
Incidence
Comprise 6-11% of renal epithelial tumors
Age
Mean: 58 years (range: 26-62 years)
Gender
M:F = 1.5:1
Presentation
Usually present as unilateral renal mass
Overwhelming majority are asymptomatic, with incidentally detected tumors following investigations for unrelated symptoms
< 1/3 present with palpable mass
Hematuria is presenting symptom in rare cases
Treatment
Surgical approaches
Partial nephrectomy surgical treatment of choice, whenever feasible
Drugs
No specific chemotherapeutic agent consistently effective in metastatic cases
Recently, targeted therapies against vascular growth factor tyrosine kinase receptors and mTOR pathway molecules have shown some rare responses
Prognosis
Prognosis of Ch-CRC better than papillary RCC in some studies and consistently better than clear cell RCC
Overall, close to 95% survival rates at 5-year follow-ups
Sarcomatoid features and perinephric extension frequently associated with aggressive clinical behavior
Other important indicators correlating with adverse clinical outcome include
Pathologic tumor stage
Large tumor size
Tumor necrosis
Overall, patients with metastatic Ch-RCC tend to do better than patients with metastasis from other common subtypes of RCC
IMAGE FINDINGS
Radiographic Findings
Usually large, well-circumscribed, unicentric renal mass
Often with features of hypovascularity
May show central scar, similar to that seen in oncocytomas and large, low-grade clear cell RCC
Presence of radiographically detected central scar offers little diagnostic information except suggesting presence of slow-growing neoplasm
MACROSCOPIC FEATURES
General Features
Characteristically, well circumscribed but not encapsulated
Cut surface homogeneous beige or pale-tan; occasionally dark brown or mahogany
Gross appearance is reflection of microscopic cell types
More brown with increasing proportion of cells with eosinophilic cytoplasm
Central scar is present in approximately 15% of tumors
Gross hemorrhage and necrosis present in 25-30%
Cystic change less common
Multifocality in < 10%
Gross involvement of renal vein seen in small number of cases
Up to 1/3 of patients may exhibit perirenal adipose tissue invasion
Size
Mean: ˜ 9 cm (range: 2-23 cm)
Largest among common subtypes of renal cell carcinoma
Mean tumor size progressively decreasing now because of earlier incidental detection on radiologic investigations for unrelated causes
Mean size in past 10-15 years has decreased to much smaller than 9 cm
MICROSCOPIC PATHOLOGY
Key Descriptors
Predominant Pattern/Injury Type
Neoplastic
Predominant Cell/Compartment Type
Epithelial
Histologic Features
Pattern of growth is predominantly solid, separated by thin, incomplete fibrovascular septa
Some tumors with variable nested, broad alveolar, solid, cystic, tubular, trabecular, or even papillary/pseudopapillary patterns
Nested/alveolar pattern usually associated with eosinophilic variants
Small percentage exhibit sarcomatoid pattern of growth
Probably the subtype with proportionately most frequent sarcomatoid differentiation among all RCCs
Microscopic foci of necrosis present in 15-25% of cases
In classic type tumors, predominant cell type is that with pale, somewhat clear-appearing cytoplasm
Unlike clear cell RCC, cytoplasm is not optically entirely clear but somewhat translucent and finely reticulated
Cytoplasm has frothy/microvesiculated appearance
Some larger cells with more voluminous clear to foamy (“hydropic”) cytoplasm often present among other “clear” cells
In eosinophilic variants, predominance of tumor cells with densely eosinophilic, granular cytoplasm
Cells with eosinophilic cytoplasm predominate in 30-40% of tumors
Most tumors show admixture of pale and eosinophilic cells
Both cell types may be juxtaposed to one another without specific patterns, or
Both cell types may have special spatial arrangement with eosinophilic cell in center and clear cells at periphery
Hyperchromatic nuclei with irregular, wrinkled outlines (“raisinoid” nuclei) is most characteristic feature
Proportion of such nuclei variable from case to case
Wrinkled nuclei more prevalent in classic types than eosinophilic variants
Another characteristic feature is presence of perinuclear cytoplasmic clarity (perinuclear halos)
While usually prominent, perinuclear halos may be only focal in some eosinophilic variants, and require careful search in such cases
Binucleated cells present in virtually all cases
Cell membranes usually appear prominent
Most cytoplasmic organelles are displaced to periphery of cytoplasm by abundant microvesicles in these tumors
This leads to impression of thick cell membranes, somewhat resembling thick cell walls in plant cells
Foci with bizarre, hyperchromatic, degenerate atypia similar to those in renal oncocytoma are common, and may be prominent in rare cases
Mitotic activity is uncommon in Ch-RCC but may be prominent in sarcomatoid and some epithelial tumors
Because of consistent presence of hyperchromatic, wrinkled, pleomorphic nuclei, Fuhrman nuclear grading is not appropriate for Ch-RCC
Currently, attempts are ongoing for clinically more relevant type-specific grading system
ANCILLARY TESTS
Histochemistry
Colloidal iron stain
Variable granular or reticular and diffuse cytoplasmic staining with Hale colloidal iron in majority of cases
Difficult stain to perform well with consistency and is highly laboratory-dependent
Focal, weak, or luminal-type staining may be seen in some cases with predominance of eosinophilic cells
Value limited in difficult cases
Immunohistochemistry
CK7 shows diffuse expression in > 75% Ch-RCC typically showing membranous accentuation
In eosinophilic variants, however, positivity is often less diffuse
Occasionally, may be present only in few clusters of cells
CD117 and Ksp-cadherin are diffusely positive in overwhelming majority
Most cases also show positivity with MOC-31, claudin-7, and EpCAM/BER-EP4/CD326
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


