Choledochoenteric Anastomosis by Choledochoduodenostomy and Other Biliary Bypass Procedures
Choledochoduoenteric anastomosis is required when stones, stricture (including bile duct injury) and malignancy necessitate permanent drainage of the bile duct. This chapter includes choledochoduodenostomy, an operation that may be performed when multiple stones have been found in the common duct at exploration and when it appears unlikely that complete removal of all stones has been achieved. It is a simple side-to-side bypass procedure. In most cases, repeated clearance of the duct by endoscopic retrograde cholangiopancreatography (ERCP) has replaced this operation.
Choledochojejunostomy and cholecystojejunostomy are performed as part of reconstruction after bile duct injury (see Chapter 76), malignancy, or as palliative procedures performed for advanced malignant disease involving the periampullary region. In choledochojejunostomy, an anastomosis of the bile duct to a loop of jejunum is performed. Cholecystojejunostomy consists of anastomosis of the gallbladder to a jejunal loop. These have largely been superseded by endoscopic stent placement.
Hepaticojejunostomy and choledochojejunostomy are also performed for reconstruction after bile duct injuries. Finally, resection of tumors of the hepatic duct bifurcation (Klatskin tumors) necessitates high reconstruction. References at the end of the chapter detail these applications.
SCORE™, the Surgical Council on Resident Education, classified choledochoenteric anastomosis as an “ESSENTIAL UNCOMMON” procedure.
HALLMARK ANATOMIC COMPLICATIONS—CHOLEDOCHODUODENOSTOMY
Sump syndrome from debris in distal duct
LIST OF STRUCTURES
Bile duct
Gallbladder
Cystic duct
Pancreas
Duodenum
Jejunum
Transverse colon
Superior mesenteric artery
Jejunal branches
Middle colic artery
STEPS IN PROCEDURE—CHOLEDOCHODUODENOSTOMY
Clean anterior surface of distal bile duct
Place two stay sutures
Make longitudinal choledochotomy low on bile duct
Perform bile duct exploration
Create transverse incision on upper aspect of duodenum, centered on choledochotomy
Construct two-layered anastomosis between duodenum and bile duct
Place omentum around anastomosis
Consider placing closed suction drains
Close abdomen in usual fashion
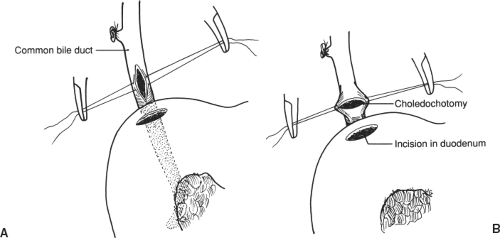 Figure 75.1 Choledochotomy and duodenotomy. A. Stay sutures placed. B. Tension placed upon stay sutures to prepare longitudinal incision for anastomosis to duodenotomy. |
Choledochoduodenostomy
Choledochotomy and Duodenotomy (Fig. 75.1)
Technical Points
Expose and prepare the bile duct for exploration, as detailed in Chapter 72. Place two stay sutures and make a longitudinal incision in the lower third of the common duct. Make the incision approximately 2 cm in length and just above the appearance of the common duct over the superior aspect of the duodenum. Place the incision lower than you normally would for common duct exploration to facilitate construction of the choledochoduodenal anastomosis. Explore the common duct thoroughly.
Anatomic Points
The close proximity of the distal bile duct and duodenum make this anastomosis possible. Extra mobility of the duodenum may be obtained by performing a Kocher maneuver.
Anastomosis (Fig. 75.2)
Technical and Anatomic Points
Place stay sutures on the anterior duodenal wall just below the entry of the bile duct into the duodenum. Center a longitudinal duodenotomy above the choledochotomy on the anterior superior surface of the duodenum. Make this incision approximately the same length as the incision in the bile duct.
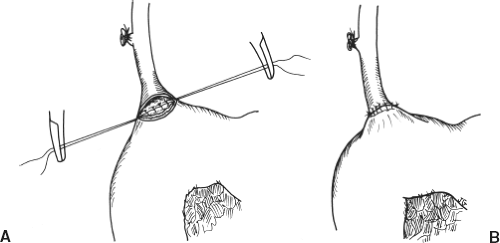 Figure 75.2 Choledochoduodenostomy—end-to-side anastomosis |
The two incisions will be perpendicular to each other and will produce a diamond-shaped opening when sutured together. Place a posterior interrupted row of 4-0 silk Lembert sutures, beginning at the apex of the choledochotomy and continuing laterally in both directions. This will form the back wall of the anastomosis. Interrupted mucosal sutures of 4-0 Vicryl can be placed if desired. Next, suture the anterior row with interrupted sutures of 4-0 Vicryl on the inner layer and interrupted 4-0 silk on the outer layer. Alternatively, a single layer of interrupted 4-0 polydioxanone (PDS) sutures may be used.
Do not stent the anastomosis or place a T-tube or other drainage device in the common duct. A lumen should be palpable to the tip of the finger at the conclusion of the procedure. Place omentum around the choledochoduodenal anastomosis and then place two closed suction drains (generally, one on each side) in the vicinity of the anastomosis.
Choledochojejunostomy
Choledochotomy and Construction of a Roux-en-Y Anastomosis (Fig. 75.3)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


