but favored locations include the upper limb, trunk, and head and neck.2 Rare examples arise within joints, especially the knee.3 There is sometimes a history of local trauma. Clinical subsets include cranial fasciitis and proliferative funiculitis,4 and the principal morphologic variants are intravascular, ossifying, and proliferative fasciitis. The typical lesion of nodular fasciitis grows rapidly over a period of weeks and then remains stable, rarely exceeding 5 cm in diameter. Most examples arise in subcutis, but the process can extend from the deep aspect of the deep fascia to involve skeletal muscle (intramuscular fasciitis) or, rarely, be sited wholly within the dermis. Nodular fasciitis is benign and, except for occasional examples of intravascular fasciitis, very rarely recurs even when incompletely excised.5 Those that do so should be carefully reviewed in case they are spindle cell sarcomas.2
TABLE 3.1 Features of Fibroblasts, Myofibroblasts, and Smooth Muscle Cells | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 3.2 Differential Diagnosis of Cellular Fibroblastic-Myofibroblastic Lesions | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
atypia should raise concern for sarcoma, notably low-grade myofibrosarcoma. The stroma is at first myxoid (Fig. 3.1, e-Fig. 3.1). Later, there is increased cellularity with a vague storiform pattern (e-Fig. 3.2). Focally, there remain small microcysts containing a few extravasated red blood cells and lymphocytes, around which the spindle cells are curved (crescent sign) (e-Figs. 3.3 and 3.4). Small multinucleated cells can also be a feature (e-Fig. 3.5).6 This is followed by fibrosis with distinct collagen bundles and fewer cells, which are more slender with wavy nuclei (e-Figs. 3.6 and 3.7). Since the different stages usually coexist in the same lesion, there is a characteristic heterogeneity or “zoning” phenomenon that is helpful for diagnosis. Occasionally there is a central cyst containing fibrin, surrounded by radial leashes of elongated capillaries.
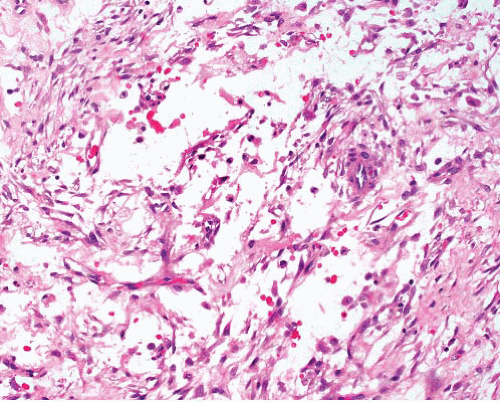 FIGURE 3.1 Nodular fasciitis. This early stage lesion shows fascicles and files of myofibroblasts in myxoid stroma. There are lymphocytes and red blood cells in the stroma. |
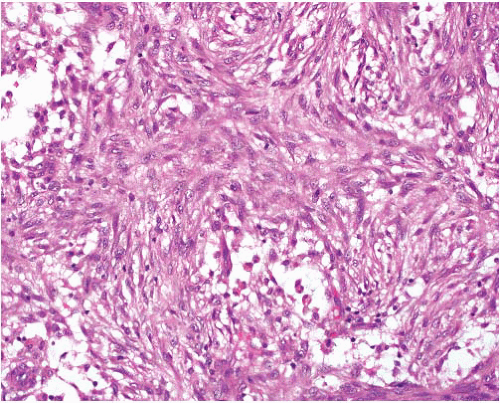 FIGURE 3.2 Nodular fasciitis. Cellular phase displays sheets of bland cells with ill-defined storiform pattern. The cells have ovoid nuclei and small nucleoli, with scattered mitoses. Note the focal stromal microcysts. |
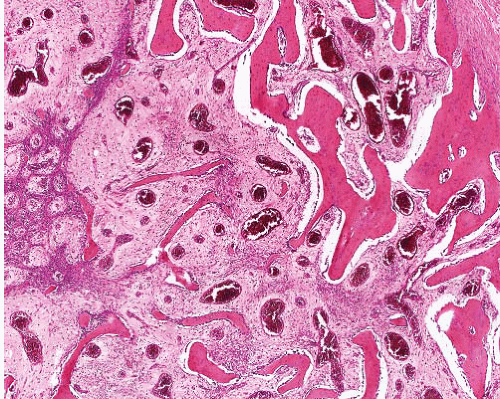 FIGURE 3.3 Ossifying fasciitis. Within a cellular background of nodular fasciitis, there is bone formation with maturation and enlargement of trabeculae from left to right imparting a zoning appearance. |
form a firm, sometimes painful, mobile subcutaneous nodule that rarely exceeds 5 cm in diameter and is usually smaller.
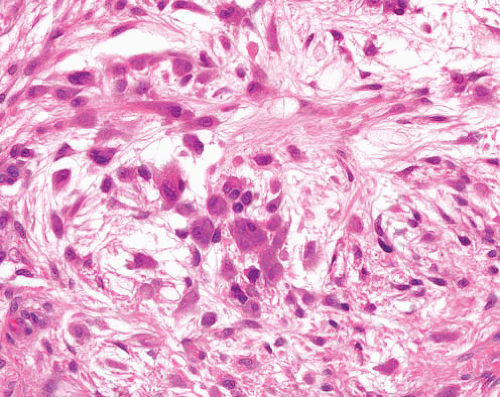 FIGURE 3.4 Proliferative fasciitis. This shows typical clusters of rounded ganglion-like cells of varying size, with abundant darkly staining cytoplasm. There are also more spindled and stellate cells, which merge with the nodular fasciitis-like background. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


