A 76-year-old man with aortoiliac occlusive disease undergoes percutaneous transluminal angioplasty of his left common iliac artery. What is the patency rate for patients who undergo angioplasty for iliac occlusive disease?
Percutaneous transluminal angioplasty for stenotic lesions in peripheral arteries is considered a viable option for patients thought to be at high risk for surgery. The use of angioplasty instead of vascular bypass avoids the risks and complications of anesthesia, and is associated with shortened hospital stays and more rapid return to normal activities. The overall patency of angioplasty for stenotic lesions is 70% to 80% at 1 year and 50% to 60% at 5 years. Complications specific to angioplasty include vascular dissection, vessel rupture, and distal embolization, which may occur up to 4% of the time.
Kudo T, Chandra FA, Ahn SS. Long-term outcomes and predictors of iliac angioplasty with selective stenting. J Vasc Surg. 2005;42:466-475.
1C02
Key word: Common Complications of Popliteal Aneurysms
Author: Robert A. Meguid, MD, MPH
Editors: G. Melville Williams, MD, FACS, and Christopher J. Abularrage, MD
A 68-year-old man presents with pain in his left leg. Examination and workup confirm diagnosis of a popliteal aneurysm. What is the most common complication that would result in the patient’s leg pain?
Aortic aneurysm rupture
Nerve impingement by the popliteal aneurysm
Popliteal aneurysm rupture
Thromboembolic events associated with the popliteal aneurysm
Answer: (D) Thromboembolic events associated with the popliteal aneurysm
Rationale:
Fifty to eighty percent of patients with popliteal aneurysms present with symptoms most commonly due to ischemia. Ischemia develops due to thrombosis of the aneurysm, distal embolization to the tibial or pedal arteries, or a combination of these. The resulting ischemia may manifest itself in a range from mild claudication to gangrene depending on the extent of thrombosis and embolization. Thromboembolism ultimately occurs in up to 35% of popliteal aneurysms if left untreated.
Less common complications of popliteal aneurysms include venous obstruction and nerve impingement due to local compression by the aneurysm. Popliteal aneurysm rupture is rare, occurring in less than 5% of patients.
Popliteal aneurysms are the most frequent site of peripheral arterial aneurysms. Ninety-five percent are caused by atherosclerosis, and they occur bilaterally 40% to 60% of the time. Of note, there is a high incidence of other concurrent aneurysms, so examination must be inclusive for abdominal, iliac, and femoral artery aneurysms. The incidence of concomitant abdominal aortic aneurysm is approximately 25%.
Diagnosis is initially clinical, with popliteal aneurysms palpable as a pulsatile or, in the case of thrombosis, firm mass. Confirmation of diagnosis on physical examination is made via ultrasound or computed tomography (CT) angiography.
Messiner R, Han DC. Popliteal and femoral artery aneurysms. In: Cameron JL, Cameron AM eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Mosby; 2011:793-798.
1C03
Key word: Advantage of Lytic Therapy for Lower-extremity Ischemia
Author: Robert A. Meguid, MD, MPH
Editors: James H. Black III, MD, FACS, and Christopher J. Abularrage, MD
A 68-year-old man with atrial fibrillation presents to the emergency room with a cool, pulseless right foot. Sensation is intact. Duplex ultrasound of the right leg reveals multiple femoral stenoses and tibioperoneal thrombosis with poor tibial flow. What is the most appropriate management?
Thrombolysis is indicated for patients with no or only mild sensorimotor deficits. Furthermore, this technique is useful when complete clot evacuation is unlikely using surgical embolectomy, or when the distal vessels are also occluded preventing inflow patency. A confirmatory angiography should be performed following intra-arterial site-directed thrombolysis.
Arterial narrowing may preclude balloon catheter placement for surgical embolectomy in some patients. In these cases, a guidewire can be passed into and through the clot, followed by an infusion catheter. Arteriography can be performed to confirm the extent of clot and to guide catheter placement. Then, lytic agents can be injected through side holes in the catheter, perfusing the clot from within.
Intra-arterial site-directed thrombolysis allows simultaneous identification of the nature of the lesion via angiography, suggesting stenting or balloon dilation of stenoses. In addition, this allows for the monitoring of progress in thrombolysis. If thrombolysis is not progressing, surgical therapy may be indicated. Thrombolysis should not be used for common femoral artery emboli.
Absolute contraindications to lytic therapy include active internal bleeding, cerebrovascular accident within 2 months, and intracranial disease. Relative contraindications include surgery or trauma within 10 days, likelihood of left heart thrombus, episodes of serious gastrointestinal bleeding within 90 days, hypertension, pregnancy, bacterial endocarditis, and diabetic hemorrhagic retinopathy.
Owings JT. Venous thromboembolism. In: Souba WW, Fink MP, Jurkovich GJ, Kaiser LR, Pearce WH, Pemberton JH, Soper NJ, eds. ACS Surgery: Principles and Practice. 4th ed. New York, NY: WebMD; 2004:719-737.
Pamoukian VN, Shortell CK. Pulseless extremity and atheroembolism. In: Souba WW, Fink MP, Jurkovich GJ, Kaiser LR, Pearce WH, Pemberton JH, Soper NJ, eds. ACS Surgery: Principles and Practice. 4th ed. New York, NY: WebMD; 2004:696-707.
1C04
Key word: Treatment of Embolus Post-myocardial Infarction
Author: Robert A. Meguid, MD, MPH
Editor: William A. Baumgartner, MD
A 73-year-old man has developed a pulseless left lower leg 8 days after experiencing a myocardial infarction (MI) requiring cardiopulmonary resuscitation. On examination, he has diminished sensation in his left foot. What is the most appropriate definitive treatment?
Answer: (D) Percutaneous embolectomy under local anesthesia
Rationale:
The most common cause of peripheral arterial embolization is atrial fibrillation, accounting for 66% to 75% of all cases. The second most common cause (20%) is MI resulting in embolization of left ventricular wall thrombus. Peripheral arterial embolization occurs in 5% of patients with mural wall thrombus, and occurs most frequently between 3 and 28 days after MI.
Treatment for the acutely ischemic limb is guided by category of limb ischemia. Initial workup includes history and physical examination, Doppler ultrasound evaluation of the threatened limb, and prompt initiation of heparin anticoagulation. Current recommendations for unfractionated heparin are an initial bolus of 80 units/kg IV, followed by infusion of 18 units/kg/hr, titrating to a goal aPTT ratio of 2. Determination of the category of limb ischemia is by physical examination and ultrasonography or angiography. Category I is occlusion of a narrowed artery with good collateral perfusion. Treatment is limited to anticoagulation. Category II is a threatened limb that may be salvaged after embolectomy. Category III is a nonsalvageable limb, requiring amputation.
Appropriate management of category II acute limb ischemia is either through emergent surgical embolectomy or intra-arterial site-directed thrombolysis. The risks of thrombolytic agents must be evaluated, especially in patients who have undergone recent cardiopulmonary resuscitation. In addition, thrombolytic agents are not indicated in patients who have sensorimotor deficits. Left heart thrombus is a relative contraindication to lytic therapy.
Embolectomy with or without revascularization is indicated in patients with sensorimotor deficits. This may be performed percutaneously or surgically. Of note, in patients having suffered recent MI, the risk of intraoperative or postoperative repeat MI is greatly increased; therefore, percutaneous embolectomy under local anesthesia is favored.
Reference:
Tucker SW, Pamoukian VN, Shortell CK. Chapter 65: Pulseless extremity and atheroembolism. In: Souba WW, Fink MP, Jurkovich GJ, Kaiser LR, Pearce WH, Pemberton JH, Soper NJ, eds. ACS Surgery: Principles and Practice. 6th ed. New York, NY: WebMD; 2007. Accessed October 12, 2011. Online Edition.
1C05
Key word: Etiology of Late Hemorrhage of Vascular Grafts
Authors: Robert A. Meguid, MD, MPH, and Susanna M. Nazarian, MD, PhD
Editor: Julie A. Freischlag, MD
Eighteen months after undergoing an aortobifemoral artery bypass, a 74-year-old man presents with a painful swelling in his left groin. Ultrasound demonstrates a pseudoaneurysm at the site of the distal anastomosis with surrounding fluid. What is the likely underlying cause of this finding?
Anastomotic disruption is the cause of delayed hemorrhage in vascular grafts. While the exact cause of disruption is usually unknown, graft infection is suspected in most cases.
Infection by virulent bacteria usually results in graft infections within 4 months of surgery. Patients develop signs of sepsis as well as evidence of local infection. Bacteria contributing to early graft infection include Staphylococcus aureus, Proteus, Klebsiella, Enterobacter, and Pseudomonas, all of which produce proteases and break down the arterial wall adjacent to the anastomosis. This results in separation of the graft from the host artery, creating a pseudoaneurysm. These may rupture, thrombose, or embolize. Less virulent bacteria such as Staphylococcus epidermidis may cause delayed graft infections. Infection of the graft may originate from septic emboli, usually from mitral or aortic valves, or from direct contamination of the graft during initial surgery. Successful treatment of graft infection includes systemic antibiotics and frequently, graft removal and revision.
Poor suture technique has been suspected as a cause of graft failure. However, studies have shown that most cases of anastomotic disruption are due to graft infection. Graft failure due to graft dilation was associated with ultra lightweight knitted Dacron grafts used in the early 1970s. This prosthetic has since been abandoned by manufacturers. Suture failure was previously found with silk sutures in vascular anastomoses. Anastomoses are currently created with more durable suture material such as polypropylene or monofilament expanded polytetrafluroethylene (ePTFE).
In a review of 307 patients who underwent abdominal aortic aneurysm (AAA) repair between 1957 and 1990 at the Mayo Clinic, 9.4% of patients had a graft-related complication. At a mean follow-up of 5.8 years, the rates of complications were as follows: Anastomotic pseudoaneurysm (3%), graft thrombosis (2%), graft-enteric erosion/fistula (1.6%), graft infection (1.3%), anastomotic hemorrhage (1.3%), colon ischemia (0.7%), and atheroembolism (0.3%). In this study, there were no complications attributable to graft failure such as dilation or rupture.
References:
Brady CM, Chaikof EL. Management of infected vascular grafts. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Mosby; 2011:857-861.
Montreuil B, Morrison L, Rosenberg L, et al. Vascular and peritoneal access. In: Souba WW, Fink MP, Jurkovich GJ, Kaiser LR, Pearce WH, Pemberton JH, Soper NJ, eds. ACS Surgery: Principles and Practice. 4th ed. New York, NY: WebMD; 2004:835.
1C06
Key word: Diagnosis of Staphylococcus Epidermidis Graft Infection
Author: Robert A. Meguid, MD, MPH
Editors: James H. Black III, MD, FACS, and Christopher J. Abularrage, MD
Eighteen months after undergoing an aortobifemoral artery bypass, a 69-year-old woman presents with a draining, cellulitic wound in her right groin, with exposed polytetrafluoroethylene (PTFE) graft. What is the most likely pathogen infecting this graft?
S. epidermidis is the most common pathogen associated with infection of implanted medical devices. Characteristically, it causes local chronic infection, but not systemic infection. S. epidermidis produces exopolysaccharides that coat the infected area. This “slime” or “biofilm” protects the bacteria from host defenses and antibiotics, allowing the S. epidermidis to propagate.
Infection by virulent bacteria usually results in graft infection within 4 months of surgery. Bacteria contributing to early graft infection include S. aureus, Proteus, Klebsiella, Enterobacter, and Pseudomonas. Less virulent bacteria such as S. epidermidis may cause delayed graft infections, often presenting over 1 year after surgery. Infection of the graft may originate from septic emboli from mitral or aortic valves, or from direct contamination of the graft during initial surgery.
Patients may present with signs of sepsis, as well as evidence of local infection, including cellulitis, draining tracts, and pulsatile masses (indicating mycotic pseudoaneurysms). Exposed graft should be assumed to be infected. In the case of aortic grafts, patients may present with sentinel gastrointestinal bleeding or major hemorrhage due to an aortoenteric fistula. Alternately, graft-enteric erosion may occur, when the graft erodes into the bowel, but the graft or anastomosis does not rupture. These patients present with chronic anemia, fever, and occult blood positive stool due to ulceration of the bowel.
Blood culture and graft culture may ultimately be positive for the infectious pathogen, but should not delay treatment. Successful treatment of graft infection includes systemic antibiotics and frequently, muscle coverage or graft excision.
References:
Brady CM, Chaikof EL. Management of infected vascular grafts. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 10th ed. Philadelphia, PA: Mosby; 2011:857-861.
Montreuil B, Morrison L, Rosenberg L, et al. Vascular and peritoneal access. In: Souba WW, Fink MP, Jurkovich GJ, Kaiser LR, Pearce WH, Pemberton JH, Soper NJ, eds. ACS Surgery: Principles and Practice. 4th ed. New York, NY: WebMD; 2004:835.
1C07
Key word: Classification of Endoleaks
Author: Babak J. Orandi, MD, MSc
Editor: Christopher J. Abularrage, MD
A 64-year-old man undergoes endovascular repair of a 5.9-cm infrarenal abdominal aortic aneurysm with bilateral iliac artery involvement. The patient does well postprocedurally and is discharged home 4 days later. A 6-month follow-up CT reveals contrast extravasation into the aneurysm sac at the proximal aspect of the aneurysm and an interval increase in the aneurysm size to 6.3 cm. What type of endoleak is described, and what is the best management?
Answer: (B) Type I endoleak; urgent endovascular repair
Rationale:
Endovascular aortic aneurysm repair (EVAR) has the advantage of sparing patients a major operation; however, the trade-off is that patients require closer surveillance and more frequent interventions. This is particularly true for patients who develop endoleak, which is defined as the persistent pressurization of the aneurysm sac that permits continued aneurysm growth and potential rupture. Endoleaks can be classified as type I to type IV and endotension, which is sometimes referred to as a type V endoleak. Type I endoleak results from an incomplete seal between the stent graft and the native vessel. Type IA is a proximal leak, while a type IB is a distal leak. Type II endoleak occurs when there is persistent flow through the aneurysm sac via branch vessels, most commonly from the inferior mesenteric artery or lumbar arteries. A separation between stent graft components that permits blood flow into the aneurysm sac is a type III endoleak. Type IV endoleak occurs when blood is able to flow through porous graft material. This type of endoleak is rarely seen with more modern stent graft devices. Endotension refers to persistent pressurization of the aneurysm sac in the absence of radiographic evidence of types I to IV endoleak.
The endoleak classification schema helps determine treatment and urgency. The type of endoleak is typically confirmed by digital subtraction angiography as this allows real time assessment of flow. Types I and III, because of the risk of aneurysm growth and rupture, typically require urgent intervention. Balloon angioplasty may help approximate the graft to the vessel wall in the case of type I endoleak. If not, a Palmaz balloon expandable stent can be placed proximally to complete the seal. Alternatively, an extension aortic cuff (type IA) or iliac extension limb (type IB) may be deployed. Type III endoleaks are repaired by deploying a stent within the current stent or utilizing a cuff if the endoleak is in the distal aspect of the stent graft. The management of type II endoleak is controversial—some have advocated a conservative approach because of the low risk of aneurysm rupture. More recent research suggests that persistent type II endoleaks (>6 months) in the presence of aneurysm sac expansion require treatment via embolization of the offending vessels or, rarely, via open ligation. Type IV endoleak typically resolves with the discontinuation of anticoagulation and is rare in the modern era of EVAR. Endotension is rarely encountered and is typically treated with either open surgical repair or deploying another stent graft into the current one if symptoms of aneurysm growth are present. For all types of endoleak, continued aneurysm growth or symptoms, such as back or abdominal pain, mandate treatment. In this question, the patient has type IA endoleak with aneurysm growth, mandating urgent intervention.
Endoleak Classification Scheme
Endoleak Type
Description of Source
I
Ineffective seal at fixation zones
A
Proximal end
B
Distal end
II
Branch vessels (e.g., intercostals, bronchials)
A
Single vessel (simple)
B
Two or more vessels creating a circuit (complex)
III
Structural endograft failure
A
Junctional separation (of modular components)
B
Endograft fracture or holes
IV
Through the stent grafts caused by porosity (<30 days)
V
Endotension (growth of aneurysm sac despite no identifiable source)
Reprinted with permission from: Lee TC, Hughes C. Complications of thoracic endovascular stent grafts. In: Franco KL, Thourani VH, eds. Cardiothoracic Surgery Review. Philadelphia, PA: Lippincott Williams & Wilkins; 2012:584.
References:
Abularrage CJ, Patel VI, Conrad MF, et al. Improved results using Onyx glue for the treatment of persistent type 2 endoleak after endovascular aneurysm repair. J Vasc Surg. 2012;56(3):630-636.
Buth J, Harris PL, van Marrewijk C, et al. The significance and management of different types of endoleaks. Semin Vasc Surg. 2003;16(2):95-102.
Heikkinen MA, Arko FR, Zarins CK. What is the significance of endoleaks and endotension? Surg Clin North Am. 2004;84(5):1337-1352.
Liaw JV, Clark M, Gibbs R, et al. Update: Complications and management of infrarenal EVAR. Eur J Radiol. 2009;71(3):541-551.
Figure
The various endoleaks are demonstrated. A: Type 1 leaks originate at either the proximal or distal attachment sites. Note the large blush of contrast outside of the graft lumen at the proximal fixation site. B: Type 2 leaks are from the collateral circulation originating in the lumbar or inferior mesenteric arteries. Note the contrast-filled limbs of the graft and the rim of contrast outside the limbs of the graft, but within the lumen of the aorta. The other computed tomography images demonstrated that the leak originated from the inferior mesenteric artery. C: Type 3 leaks are caused by fabric tears or problems at the graft interfaces of the modular devices. Note the contrast blush outside of the lumen of the graft at the modular interface. D: Type 4 leaks are usually transient (<24 hours) trans-graft extravasations and can result from the porosity of the graft and needle holes. Reprinted with permission from: Huber TS, Lee WA. Abdominal aortic aneurysms. In: Mulholland MW, Lillemoe KD, Doherty GM, Maier RV, Upchurch GR, eds. Greenfield’s Surgery: Scientific Principles & Practice. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1743.
1C08
Key word: Etiology of Late Death after Heart Transplant
Author: Robert A. Meguid, MD, MPH
Editor: William A. Baumgartner, MD
What is the most common cause of late death after heart transplant?
While acute graft rejection is the most common cause of death within the first year after cardiac transplantation, accelerated atherosclerosis leading to myocardial infarction is the most common cause of death thereafter.
CMV infection is associated with accelerated atherosclerosis, but itself is not the cause of death. Fungal infections occur in 7% to 15% of cardiac transplantations, characteristically within the first few months. The death rate from ventilator-associated pneumonia early after transplant is approximately 20% to 30% in ventilated patients.
Willerson JT. Acute myocardial infarction. In: Wyngaarden JB, Smith LH, eds. Cecil Textbook of Medicine. 18th ed. Philadelphia, PA: W.B. Saunders; 1988:330.
1C09
Key word: Adjuncts to Improve Vascular Graft Patency
Author: Susanna M. Nazarian, MD, PhD
Editor: Julie A. Freischlag, MD
A 72-year-old man is seen in clinic preoperatively to prepare for his upcoming femoral-tibial artery bypass for vascular insufficiency. The duplex scan demonstrates poor candidates for venous conduits, so the use of synthetic graft is anticipated. The long-term outcome for this patient could be improved by:
Clopidogrel use for the first 3 months after surgery
Daily use of 81-mg aspirin indefinitely
Low-molecular-weight heparin injections for the first 6 weeks after surgery
The use of support stockings
Warfarin use with a goal International Normalization Ratio (INR) of 1.5
Answer: (B) Daily use of 81-mg aspirin indefinitely
Rationale:
Aspirin has demonstrated efficacy in maintaining graft patency following infrainguinal prosthetic bypass in multiple randomized clinical trials. In addition, statins may enhance graft patency following bypass surgery. Anticoagulation with warfarin should be reserved for patients at high risk for clotting, while the use of clopidogrel after prosthetic grafting remains undefined. Preliminary data suggest that aspirin in combination with clopidogrel may provide superior patency results, though further studies are necessary.
The multicenter, prospective Dutch Bypass Oral Anticoagulants or Aspirin (BOA) trial randomized 2,690 lower-extremity bypass patients to anticoagulation to INR 3 to 4.5 or 80-mg aspirin daily. In subgroup analysis for prosthetic grafts, patients receiving aspirin had improved graft patency compared with patients receiving anticoagulation. Conversely, vein graft patients fared better in the anticoagulation arm. In combined analysis for both prosthetic and vein, the patency rates were not significantly different for the two therapies. A Veterans Affairs Cooperative trial compared aspirin to aspirin and warfarin (goal INR 1.4 to 2.8), and found no improvement in those receiving the additional warfarin. Predictably, patients receiving warfarin in both studies suffered twice as many hemorrhagic events. Statins were found to decrease the risk of vein graft failure by 3.2 times in a retrospective study of 172 patients.
Five-year patency rates for infrainguinal bypass are inferior to those seen with aortofemoral bypasses, ranging from 15% for bypasses to the tibial artery using prosthetic graft, to 80% for bypasses to the popliteal artery using saphenous vein.
References:
Dagher NN, Modrall JG. Pharmacotherapy before and after revascularization: Anticoagulation, antiplatelet agents, and statins. Seminars in Vascular Surgery. 2007;20:10-14.
Jackson AJ, Coats P, Orr DJ, et al. Pharmacotherapy to improve outcomes in infrainguinal bypass graft surgery: A review of current treatment strategies. Annals of Vascular Surgery. 2010;24:562-572.
Liem TK, Silver D. Role of antithrombotic drugs in maintaining graft patency. In: Ernst CB, Stanley JC, eds. Current Therapy in Vascular Surgery. 4th ed. St. Louis, MO: Mosby; 2001:546-548.
1C10
Key word: Characteristics of Thoracic Outlet Syndrome
Author: Robert A. Meguid, MD, MPH
Editor: Julie A. Freischlag, MD
A 28-year-old female professional violinist presents with headaches, neck pain, and hand clumsiness in her right hand. She also reports occasional numbness in the hand and right-sided chest pain. Which of the following is the likely cause of her symptoms?
All of the symptoms described in the question are due to TOS. TOS is a constellation of neurovascular symptoms attributed to compression of the subclavian artery and vein, as well as the brachial plexus and sympathetic chain as they run over the first rib. The structures that may cause compression include the scalenus anticus and medius, pectoralis minor, and subclavius muscles, costocoracoid ligament, costoclavicular membrane, and cervical ribs.
Symptoms are attributed to nerve compression, arterial compression, sympathetic compression, and/or venous compression. Ninety-five percent of patients present with pain and paresthesias, of which most involve the ulnar nerve. Arterial compression may present as an incidental finding, and is associated with aneurysm proximal to the outlet compression. Alternately, patients may present with thrombosis and distal embolization, requiring surgical intervention. Sympathetic compression results in chest, neck, shoulder, arm, and hand pain. This often simulates angina pectoris, and is termed “pseudoangina.” Additional potential symptoms resulting from sympathetic compression include Raynaud phenomenon and reflex sympathetic dystrophy. Venous compression (Paget-Schroetter Syndrome) is rare, results in effort thrombosis of the axillary subclavian vein, and occurs due to repetitive muscular activity or trauma.
Initial treatment of neurologic symptoms entails conservative measures including physical therapy. Failure of conservative treatment in the face of persisting symptoms necessitates surgery. Patients with neurologic complaints should undergo nerve conduction velocity (NCV) studies of the ulnar or median nerve across the thoracic outlet. Normal values are greater than 85 m/sec. Patients with values of 60 to 85 m/sec should respond to conservative therapy consisting of physical therapy; however, patients with NCVs less than 60 m/sec usually require surgery.
Arterial compression should be confirmed with ultrasonography and arteriography. Patients with aneurysms should undergo first or cervical rib resection, and thrombectomy and/or embolectomy, aneurysm repair, and dorsal sympathectomy as necessary.
In diagnosing sympathetic compression resulting in “pseudoangina,” workup includes ruling out coronary artery disease via coronary angiogram. First rib resection for neurovascular symptoms usually resolves pain and other associated symptoms from sympathetic compression.
Treatment of venous compression is resection of the first rib, costoclavicular ligament medially, and the scalenus anticus muscle.
Reference:
Urschel H. Thoracic outlet syndrome. In: Yang SC, Cameron DE, eds. Current Therapy in Thoracic and Cardiovascular Surgery. Philadelphia, PA: Mosby; 2004:272-275.
1C11
Key word: Treatment of Occlusion of the Common Iliac Artery in Patients with COPD
Author: Robert A. Meguid, MD, MPH
Editor: Julie A. Freischlag, MD
An 82-year-old man with a history of severe chronic obstructive pulmonary disease (COPD) presents with claudication and is found to have occlusive disease localized to the left common iliac artery. Which of the following procedures is the most appropriate for management of this patient’s disease?
Anticoagulation using intravenous heparin
Aortobifemoral artery bypass with synthetic graft
Conservative treatment
Femoral to femoral artery bypass with venous autograft
Percutaneous transluminal angioplasty (PTA) under local anesthesia
Answer: (E) Percutaneous transluminal angioplasty (PTA) under local anesthesia
Rationale:
COPD is the fifth leading cause of death in the United States. It is associated with multiple perioperative complications, including failure to extubate postoperatively and prolonged postoperative mechanical ventilation.
Patients with iliac arterial occlusion present with absent pulses in the ipsilateral leg, as well as claudication-type pain. Diagnosis is confirmed with arteriography. While a bypass graft may be indicated in a healthier patient, it would be prudent to avoid an operation necessitating intubation in this scenario.
PTA under local anesthesia, with or without placement of a stent into the artery, would be a viable option here. The average success rate of PTA for treatment of total occlusion of the iliac artery is 65% with a 2- to 4-year patency rate of 75% to 100%.
Anticoagulation using intravenous heparin is inadequate definitive therapy for the occlusion of the iliac artery. Aortobifemoral artery bypass with PTFE graft would be indicated in a patient with occlusive disease of the abdominal aorta and/or bilateral iliac arteries. In this example, aortobifemoral artery bypass would not be the best option given the patient’s comorbidities and the limited extent of disease.
Tucker SW, Pamoukian VN, Shortell CK. Chapter 65: Pulseless extremity and atheroembolism. In: Souba WW, Fink MP, Jurkovich GJ, Kaiser LR, Pearce WH, Pemberton JH, Soper NJ, eds. ACS Surgery: Principles and Practice. 6th ed. New York, NY: WebMD; 2007. http://www.acssurgery.com/acssurgery/institutional/instTableOfContent.action. Accessed October 14, 2011. Online Edition.
1C12
Key word: Treatment of Air Embolus
Author: Babak J. Orandi, MD, MSc
Editor: Christopher M. Sciortino, MD, PhD
A previously healthy 63-year-old woman began to complain of increased shortness of breath and chest pain while undergoing a root canal. After stopping the procedure, her symptoms resolved, and the oral surgeon resumed drilling. She began experiencing right facial pain and periorbital and neck swelling and subsequently complained of severe dyspnea. The patient’s blood pressure then became undetectable. An emergent ECG showed nonspecific ST wave changes. Her pulse oximeter revealed an oxygen saturation of 89% to 90% throughout the procedure. Immediate action should be?
Answer: (E) Position the patient in left lateral decubitus Trendelenburg position
Rationale:
Venous gas embolism (VGE) occurs when gas is introduced into the systemic venous circulation. This requires that the pressure gradient be such that air entry into the vessel is promoted over the egress of blood. A rare occurrence, VGE is typically iatrogenic, and while room air is the most common agent, any gas used medically can be causative (CO2, NO2, N2, etc.).
Once in the venous circulation, the gas embolism travels to the right heart and enters the pulmonary arterial circulation, leading to impaired gas exchange, dysrhythmias, and pulmonary hypertension. The latter can cause acute right heart strain and subsequent heart failure. The classic scenario in which VGE occurs is in the placement or use of central venous or hemodialysis catheters, though it can be seen in a variety of other situations, including trauma, childbirth, and craniotomy. Auscultation may demonstrate the classic finding of a churning murmur (“mill-wheel” murmur) that is present throughout systole and diastole. Other signs include jugular venous distension, dyspnea, chest pain, mental status changes, and cardiovascular collapse.
In the instance of mental status changes or any neurologic signs, it must be assumed that the patient developed a paradoxical embolism, most commonly through a patent foramen ovale, with conversion of the VGE to an arterial gas embolism (AGE). While treatment for both involves prevention of further embolization, supportive care, resuscitation, intubation, 100% oxygen administration, and a possible role for hyperbaric oxygen therapy, the immediate positioning of the patient differs based on whether or not the embolism is venous or arterial in nature. VGE patients should immediately be placed in the left lateral decubitus and Trendelenburg (head down) position, with the goal of maintaining the embolus in the right ventricle and preventing it from traveling into the pulmonary circulation. Because arterial flow is stronger, this position will not prevent AGE from traveling distally to the heart and brain where it will disrupt flow. The Trendelenburg position may also exacerbate cerebral swelling associated with AGE to the brain; accordingly, the preferred position for AGE is in the flat supine position.
Isolated case reports and some animal experiments have suggested that for patients with VGE, evacuation of the embolism may be possible through a central venous catheter, though this is typically only done if the patient already has a catheter in place; rarely is the volume evacuated sufficient to achieve clinical improvement.
References:
Jorens PG, Van Marck E, Snoeckz A, et al. Nonthrombotic pulmonary embolism. Eur Respir J. 2009;34(2):452-474.
Muth CM, Shank ES. Gas embolism. N Engl J Med. 2000;342(7):476-482.
Palmon SC, Moore LE, Lundberg J, et al. Venous air embolism: A review. J Clin Anesth. 1997;9:251-257.
1C13
Key word: Hypovolemic Shock
Author: Susanna M. Nazarian, MD, PhD
Editors: Duke E. Cameron, MD, and Christopher M. Sciortino, MD, PhD
A 24-year-old man presents to the emergency department after sustaining two gunshots through his chest. Which of the following would suggest that he has lost 30% to 40% of his blood volume?
HR 90, normal blood pressure, normal or increased pulse pressure, urine output >30 mL/hr
Answer: (D) HR >120, decreased blood pressure, very decreased pulse pressure, respiratory rate 30 to 40, urine output 5 to 15 mL/hr
Rationale:
This patient is in stage III hypovolemic shock, having lost 30% to 40% of his blood volume. A 70-kg man is estimated to have 4,900 mL of blood volume, or 70-mL blood per kg of ideal body weight. The hypovolemic shock classification helps guide treatment and prognostication.
Stage I: ≤15% blood volume lost (≤750 mL), HR < 100, normal BP, normal pulse pressure, respiratory rate 14 to 20, urine output >30 mL/hr. Slightly anxious, pale, cool skin. Treat with crystalloid.
Stage II: 15% to 30% blood volume lost (750 to 1,500 mL), HR > 100, normal blood pressure, narrowed pulse pressure, orthostasis, respiratory rate 20 to 30, urine output 20 to 30 mL/hr. Anxious. Treat with crystalloid.
Stage III: 30% to 40% blood volume lost (1,500 to 2,000 mL), HR > 120, decreased blood pressure, very decreased pulse pressure, respiratory rate 30 to 40, urine output 5 to 15 mL/hr. Anxious and confused. Decreased perfusion of vital organs such as kidneys, liver, and intestines. Treat with blood and crystalloid.
Stage IV: >40% lost (>2,000 mL), HR >140, very decreased blood pressure, respiratory rate >35, negligible urine output. Confused and lethargic. Decreased perfusion of the brain and heart. Treat with blood and crystalloid.
Other types of shock include neurogenic, cardiogenic, and vasogenic shock. At the cellular level, shock is characterized by insufficient oxygen delivery (inadequate end-organ perfusion). An adrenergic response ensues within minutes, leading to tachycardia, vasoconstriction (i.e., decreased pulse pressure), and decreased renal blood flow (leading to low urine output).
 10% at 5 years
10% at 5 years 20% at 5 years
20% at 5 years 30% at 5 years
30% at 5 years 60% at 5 years
60% at 5 years 80% at 5 years
80% at 5 years Aortic aneurysm rupture
Aortic aneurysm rupture Nerve impingement by the popliteal aneurysm
Nerve impingement by the popliteal aneurysm Popliteal aneurysm rupture
Popliteal aneurysm rupture Thromboembolic events associated with the popliteal aneurysm
Thromboembolic events associated with the popliteal aneurysm Venous obstruction by the popliteal aneurysm
Venous obstruction by the popliteal aneurysm Amputation
Amputation Diagnostic angiography
Diagnostic angiography Intra-arterial site-directed thrombolysis
Intra-arterial site-directed thrombolysis Percutaneous embolectomy under local anesthesia
Percutaneous embolectomy under local anesthesia Systemic anticoagulation only
Systemic anticoagulation only Amputation
Amputation Anticoagulation using intravenous heparin
Anticoagulation using intravenous heparin Intra-arterial site-directed thrombolysis
Intra-arterial site-directed thrombolysis Percutaneous embolectomy under local anesthesia
Percutaneous embolectomy under local anesthesia Surgical bypass
Surgical bypass Atheroembolism
Atheroembolism Graft failure
Graft failure Graft infection
Graft infection Graft thrombosis
Graft thrombosis Suture failure
Suture failure Enterobacter cloacae
Enterobacter cloacae Klebsiella pneumoniae
Klebsiella pneumoniae Pseudomonas aeruginosa
Pseudomonas aeruginosa Staphylococcus aureus
Staphylococcus aureus Staphylococcus epidermidis
Staphylococcus epidermidis Type I endoleak; observation
Type I endoleak; observation Type I endoleak; urgent endovascular repair
Type I endoleak; urgent endovascular repair Type II endoleak; urgent open surgical repair
Type II endoleak; urgent open surgical repair Type III endoleak; observation
Type III endoleak; observation Type III endoleak; urgent endovascular repair
Type III endoleak; urgent endovascular repair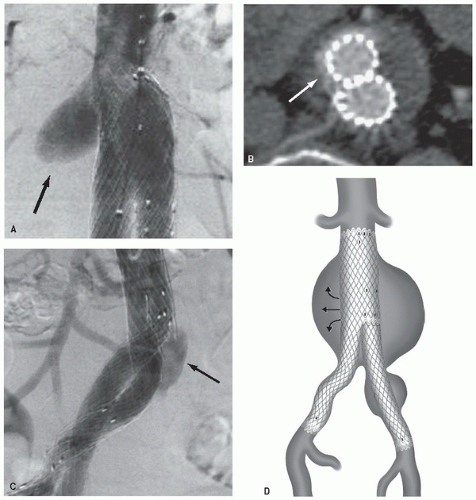
 Acute graft rejection
Acute graft rejection Accelerated atherosclerosis
Accelerated atherosclerosis Cytomegalovirus (CMV) infection
Cytomegalovirus (CMV) infection Fungal infection
Fungal infection Ventilator-associated pneumonia
Ventilator-associated pneumonia Clopidogrel use for the first 3 months after surgery
Clopidogrel use for the first 3 months after surgery Daily use of 81-mg aspirin indefinitely
Daily use of 81-mg aspirin indefinitely Low-molecular-weight heparin injections for the first 6 weeks after surgery
Low-molecular-weight heparin injections for the first 6 weeks after surgery The use of support stockings
The use of support stockings Warfarin use with a goal International Normalization Ratio (INR) of 1.5
Warfarin use with a goal International Normalization Ratio (INR) of 1.5 Carpal tunnel syndrome
Carpal tunnel syndrome Coronary artery disease
Coronary artery disease Osteoarthritis
Osteoarthritis Paget-Schroetter syndrome
Paget-Schroetter syndrome Thoracic outlet syndrome (TOS)
Thoracic outlet syndrome (TOS) Anticoagulation using intravenous heparin
Anticoagulation using intravenous heparin Aortobifemoral artery bypass with synthetic graft
Aortobifemoral artery bypass with synthetic graft Conservative treatment
Conservative treatment Femoral to femoral artery bypass with venous autograft
Femoral to femoral artery bypass with venous autograft Percutaneous transluminal angioplasty (PTA) under local anesthesia
Percutaneous transluminal angioplasty (PTA) under local anesthesia Administration of intravenous fluids
Administration of intravenous fluids Bilateral tube thoracostomy placement
Bilateral tube thoracostomy placement Initiation of intravenous antibiotics
Initiation of intravenous antibiotics Intravenous heparin therapy and/or thrombolytic therapy
Intravenous heparin therapy and/or thrombolytic therapy Position the patient in left lateral decubitus Trendelenburg position
Position the patient in left lateral decubitus Trendelenburg position HR 90, normal blood pressure, normal or increased pulse pressure, urine output >30 mL/hr
HR 90, normal blood pressure, normal or increased pulse pressure, urine output >30 mL/hr HR 110, normal blood pressure, increased pulse pressure, urine output >30 mL/hr
HR 110, normal blood pressure, increased pulse pressure, urine output >30 mL/hr HR 110, normal blood pressure, narrowed pulse pressure, urine output 20 to 30 mL/hr
HR 110, normal blood pressure, narrowed pulse pressure, urine output 20 to 30 mL/hr HR > 120, decreased blood pressure, very decreased pulse pressure, respiratory rate 30 to 40, urine output 5 to 15 mL/hr
HR > 120, decreased blood pressure, very decreased pulse pressure, respiratory rate 30 to 40, urine output 5 to 15 mL/hr HR > 140, very decreased blood pressure, respiratory rate >35, negligible urine output
HR > 140, very decreased blood pressure, respiratory rate >35, negligible urine output


