Cardiac arrhythmias
Abnormal electrical conduction or automaticity changes heart rate and rhythm in cardiac arrhythmias, also called cardiac dysrhythmias. (See Types of cardiac arrhythmias.)
Arrhythmias vary in severity, from those that are mild, asymptomatic, and require no treatment (such as sinus arrhythmia, in which the heart rate increases and decreases with respirations) to catastrophic ventricular fibrillation, which necessitates immediate resuscitation.
Arrhythmias are generally classified according to their origin (ventricular or supraventricular). Their effect on cardiac output and blood pressure, partially influenced by the site of origin, determines their clinical significance.
Causes
Arrhythmias may be congenital, or they may result from one of several factors, including myocardial ischemia, a myocardial infarction, and organic heart disease. Drug toxicity or degeneration of the conductive tissue necessary to maintain normal heart rhythm (sick sinus syndrome) sometimes can also precipitate arrhythmias.
Special considerations
If the patient isn’t being monitored, assess him for rhythm disturbances.
If the patient’s pulse is abnormally rapid, slow, or irregular, watch for signs of hypoperfusion, such as hypotension and diminished urine output.
If the patient is being monitored, document any arrhythmias and assess him for possible causes and effects.
When life-threatening arrhythmias develop, rapidly assess the level of consciousness, respirations, and pulse rate.
Initiate cardiopulmonary resuscitation, if indicated.
Evaluate the patient for altered cardiac output resulting from arrhythmias.
Administer medications as needed, and prepare for any necessary medical procedures (for example, cardioversion).
Monitor patient for predisposing factors—such as fluid and electrolyte imbalance—and signs of drug toxicity, especially digoxin toxicity. If the patient is experiencing drug toxicity, the next dose may have to be withheld.
To prevent arrhythmias in a postoperative cardiac patient, provide adequate oxygen and reduce the heart’s workload, while carefully maintaining metabolic, neurologic, respiratory, and hemodynamic status.
To avoid temporary pacemaker malfunction, install a fresh battery before each insertion. Carefully secure the external catheter wires and the pacemaker box. Assess the threshold daily. Watch closely for premature contractions, a sign of myocardial irritation.
To avert permanent pacemaker malfunction, restrict the patient’s activity after insertion. Monitor the pulse rate regularly, and watch for signs of decreased cardiac output.
If the patient has a permanent pacemaker, warn him about environmental hazards, as indicated by the pacemaker manufacturer.
Although hazards may not present a problem, 24-hour Holter monitoring may be helpful in diagnosing dysfunction.
Tell the patient to report light-headedness or syncope, and stress the importance of regular checkups.
Types of cardiac arrythmias
This chart reviews many common cardiac arrhythmias and outlines their features, causes, and treatments. Use a normal electrocardiogram strip, if available, to compare normal cardiac rhythm configurations with the rhythm strips below. Characteristics of normal rhythm include:
ventricular and atrial rates of 60 to 100 beats/minute
regular and uniform QRS complexes and P waves
PR interval of 0.12 to 0.2 second
QRS duration < 0.12 second
identical atrial and ventricular rates, with constant PR interval.
| Arrhythmia and Features | Causes | Treatment |
|---|---|---|
Sinus arrhythmia
|
|
|
Sinus tachycardia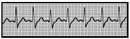
|
|
|
Sinus bradycardia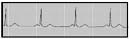
|
|



