Brachytherapy Catheter Insertion for Breast Cancer
Peter D. Beitsch
DEFINITION
Breast conservation therapy (BCT) requires postlumpectomy radiation.
Radiation can be given to the entire breast as whole breast irradiation (WBI) or to the area at the highest risk of recurrence—the breast tissue surrounding the lumpectomy cavity—by accelerated partial breast irradiation (APBI).
APBI can be delivered from an external source (3-D conformal) or an internal source (brachytherapy).
DIFFERENTIAL DIAGNOSIS
Brachytherapy can be delivered via multiple inserted catheters (interstitial multicatheter; FIG 1) or via a single insertion/multiple catheter device (FIGS 2, 3, 4) (see videos 1 and 2 in the accompanying eBook).

FIG 1 • Multiple catheter interstitial brachytherapy.

FIG 2 • Strut-adjusted volume implant (SAVI)—single insertion multicatheter strut-based device. ©Cianna Medical, Inc.
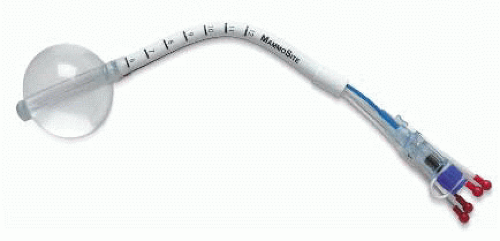
FIG 3 • MammoSite ML—single insertion multicatheter balloon device.
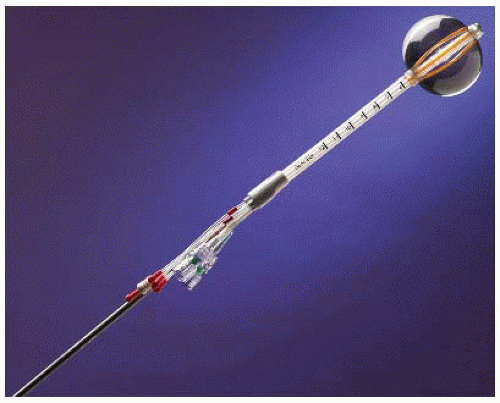
FIG 4 • Contura—single insertion multicatheter balloon device.
Radiation oncologists usually perform the multiple catheter insertions and surgeons insert the single insertion/multiple catheter devices (which is the focus of this chapter).
PATIENT HISTORY AND PHYSICAL FINDINGS
IMAGING AND OTHER DIAGNOSTIC STUDIES
Controversy exists whether all patients undergoing APBI should get preoperative advanced breast imaging (magnetic resonance imaging [MRI] or positron emission mammography); however, most surgeons only do so selectively.
Ultrasound skills by the surgeon are helpful for insertion but are not mandatory.
Table 1: Patient Selection Guidelines for Accelerated Partial Breast Irradiation | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
SURGICAL MANAGEMENT
Brachytherapy devices are routinely placed in the surgeon’s office.
Cavity evaluation devices (CEDs) (FIG 5) can be inserted at the time of the lumpectomy as a “space holder” until exchanged in the office for the brachytherapy device.
Preoperative Planning
Preoperative consultation with the radiation oncologist will be helpful in facilitating postoperative treatment scheduling.
Postlumpectomy placement in the office begins with the preoperative plan for the lumpectomy including
Location of incisions (do not perform sentinel lymph node biopsy through the lumpectomy incision)
Use of oncoplastic techniques (minimal flap rearrangement is okay but major flap movement with obliteration of the lumpectomy cavity negates the use of APBI)
Thicker wound closure if possible (more tissue between skin and cavity may require skin resection and multilayer closure)
Table 2: American Society of Radiation Oncology Consensus Statement on Patient Selection for Accelerated Partial Breast Irradiation | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


