|
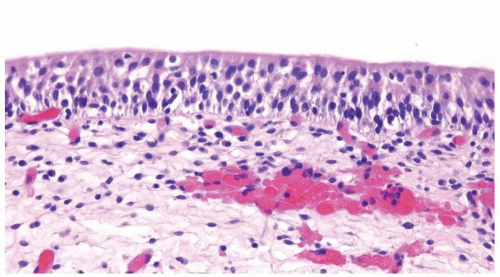 Figure 3.1.1 Normal urothelium. |
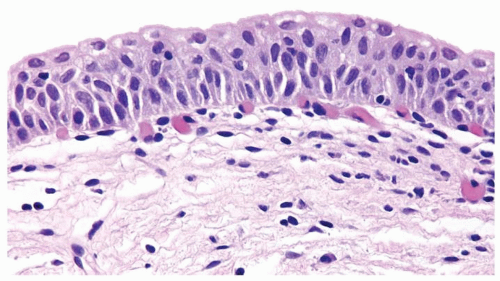 Figure 3.1.2 Urothelium with slight variation in nuclear size still consistent with normal. |
 Figure 3.1.3 Normal urothelium with slight variation in polarity but lacking nuclear atypia. |
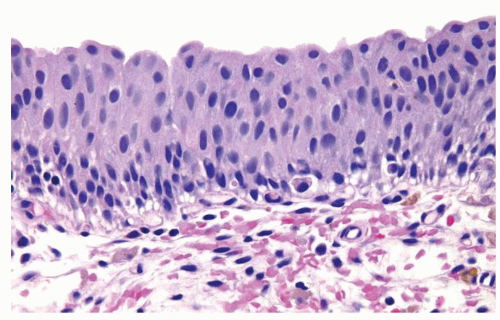 Figure 3.1.4 Dysplasia with scattered mildly enlarged hyperchromatic nuclei. |
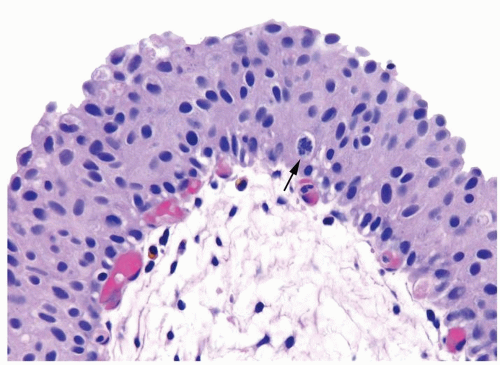 Figure 3.1.5 Dysplasia with scattered mildly enlarged hyperchromatic nuclei and mitotic figures (arrow). |
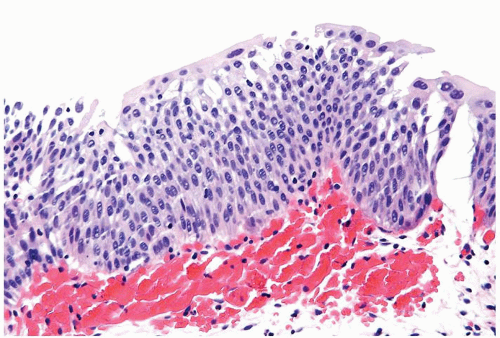 Figure 3.1.6 Dysplasia with a thickened urothelium and diffuse mildly enlarged hyperchromatic nuclei. |
|
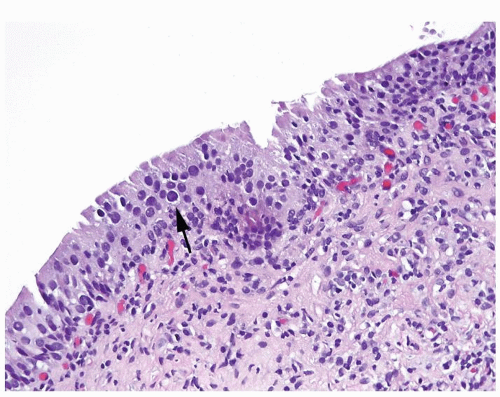 Figure 3.2.1 Dysplasia with scattered, mildly enlarged hyperchromatic nuclei (arrow). |
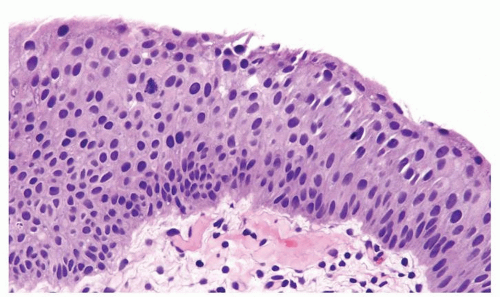 Figure 3.2.2 Dysplasia with scattered, mildly enlarged hyperchromatic nuclei. |
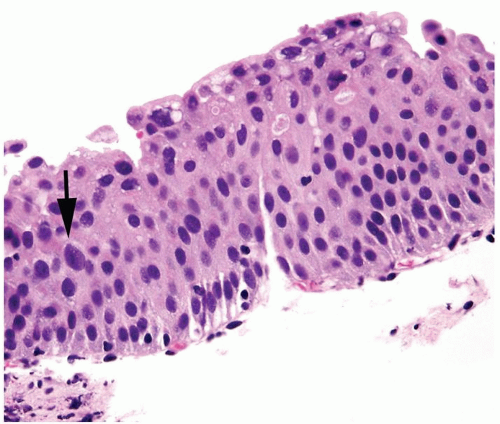 Figure 3.2.3 Dysplasia with scattered, mildly enlarged hyperchromatic nuclei (arrow). |
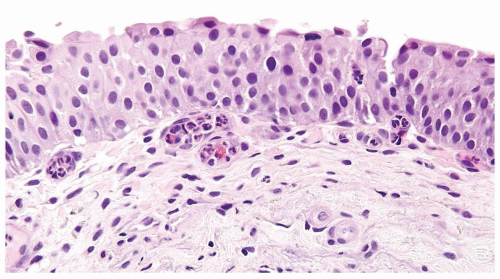 Figure 3.2.4 Dysplasia with scattered, mildly enlarged hyperchromatic nuclei. |
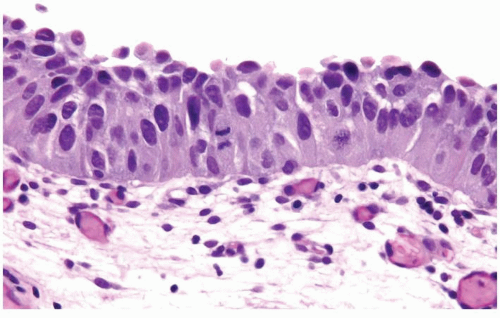 Figure 3.2.5 CIS with markedly enlarged hyperchromatic nuclei relative to stromal lymphocytes. Cells have abundant cytoplasm and a mitotic figure. |
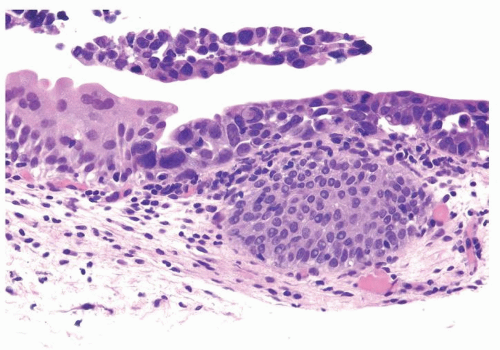 Figure 3.2.6 CIS with markedly enlarged hyperchromatic nuclei relative to the normal urothelium in von Brunn nest. |
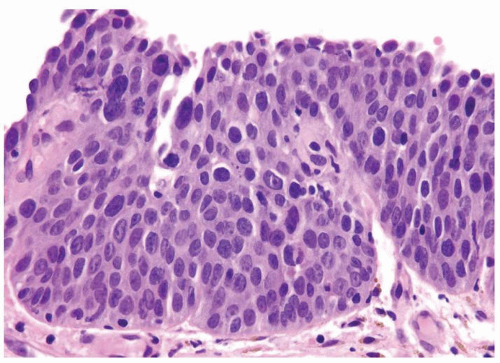 Figure 3.2.7 CIS with variably sized and shaped nuclei. Largest nuclei are markedly enlarged relative to stromal lymphocytes. |
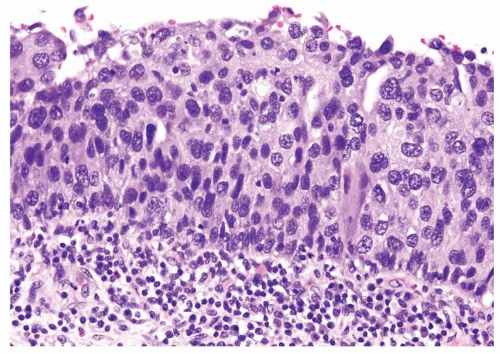 Figure 3.2.8 CIS with a thickened urothelium with diffusely enlarged and hyperchromatic nuclei. |
|
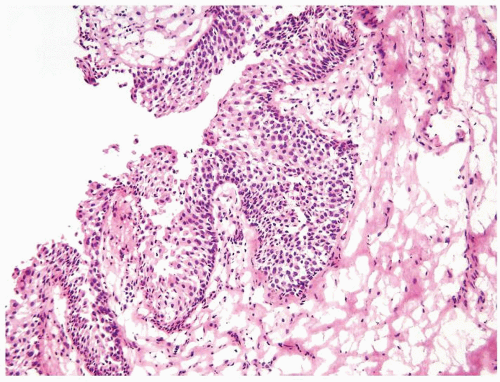 Figure 3.3.1 Benign ureteral margin at frozen section. All images in this chapter are taken at the same magnification of 10× lens. |
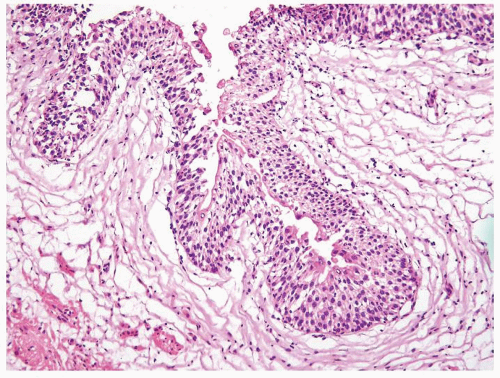 Figure 3.3.2 Benign ureteral margin at frozen section. |
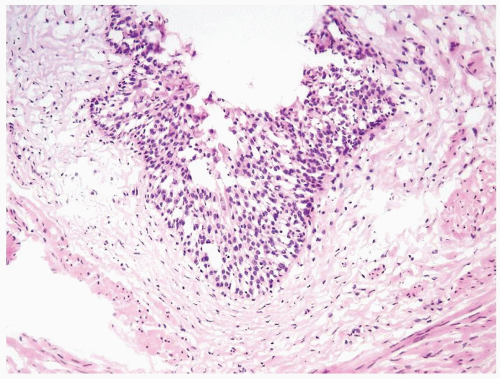 Figure 3.3.3 Benign ureteral margin at frozen section with hyperplastic appearance possibly due to tangential sectioning. |
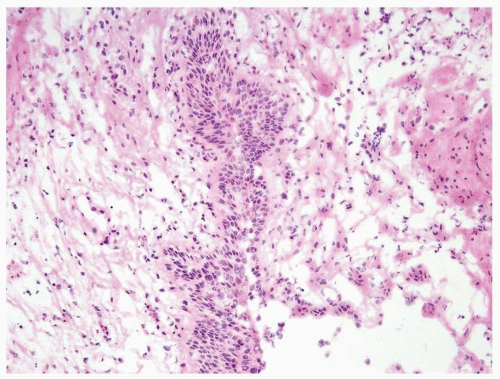 Figure 3.3.4 Benign ureteral margin at frozen section with an air-drying artifact giving rise to an appearance of slightly enlarged nuclei. |
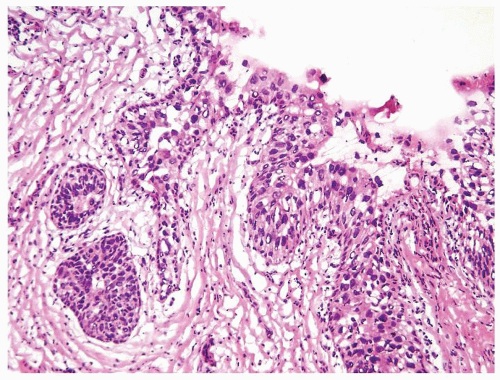 Figure 3.3.5 CIS with overtly enlarged and hyperchromatic nuclei. |
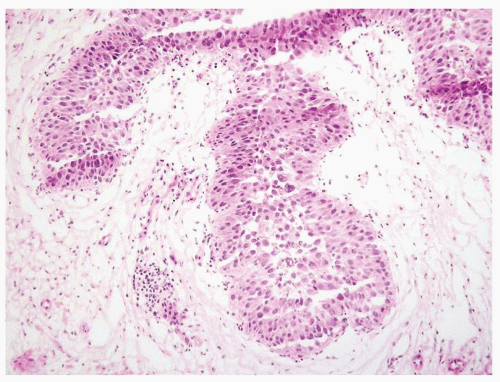 Figure 3.3.6 CIS with overtly enlarged and hyperchromatic nuclei. |
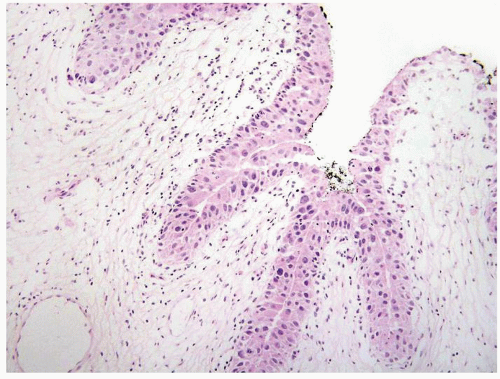 Figure 3.3.7 CIS with overtly enlarged and hyperchromatic nuclei. |
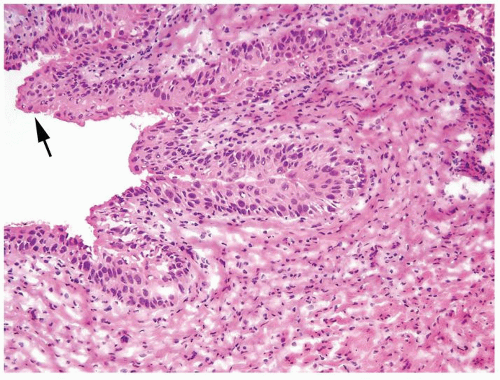 Figure 3.3.8 More difficult case where it is borderline CIS, but there is still sufficient nuclear enlargement compared to the more normal urothelium (arrow) to ask the urologist to resect more ureter in an attempt to obtain a normal urothelium. |
|
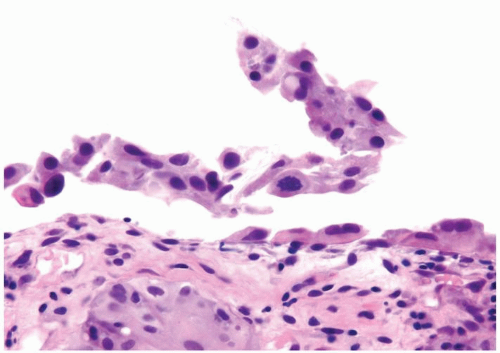 Figure 3.4.1 CIS with lifting of the urothelium from the basement membrane. |
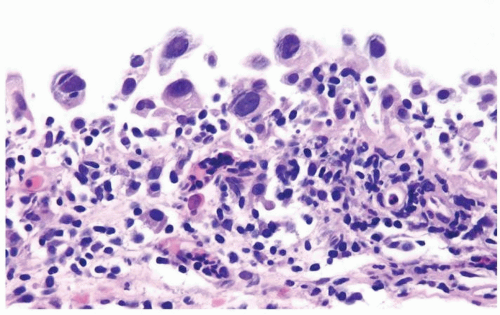 Figure 3.4.2 CIS with loosely cohesive cells with markedly enlarged hyperchromatic nuclei. |
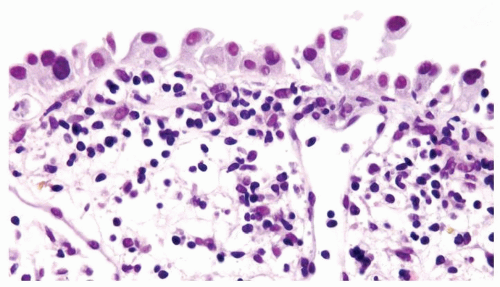 Figure 3.4.3 CIS with loosely cohesive cells with markedly enlarged hyperchromatic nuclei. The largest nucleus (left) is four to five times the size of lymphocytes. |
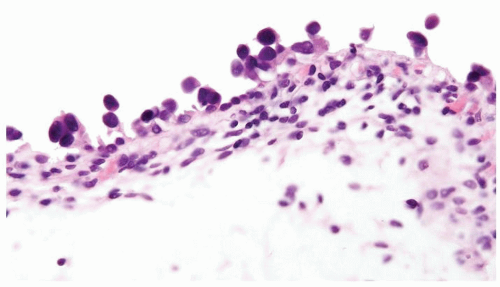 Figure 3.4.4 CIS with loosely cohesive cells with markedly enlarged hyperchromatic nuclei. |
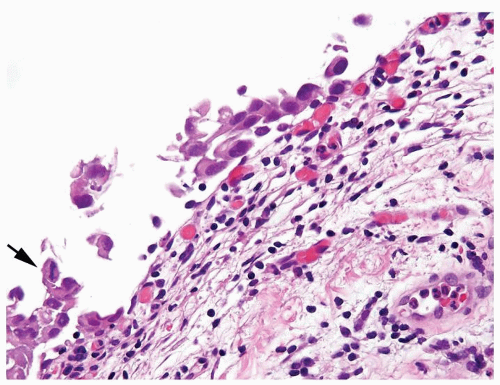 Figure 3.4.5 CIS with loosely cohesive cells with markedly enlarged hyperchromatic nuclei and mitotic figures (arrow). |
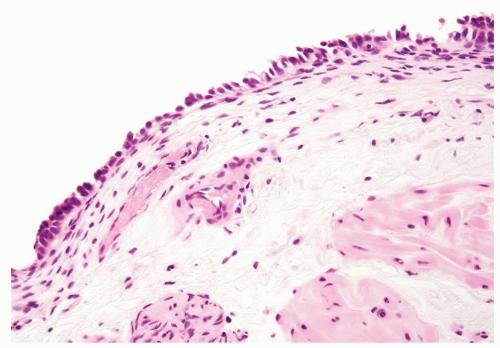 Figure 3.4.6 Benign urothelium with denudation. The remaining urothelium consists of cells with relatively small uniform nuclei. |
|
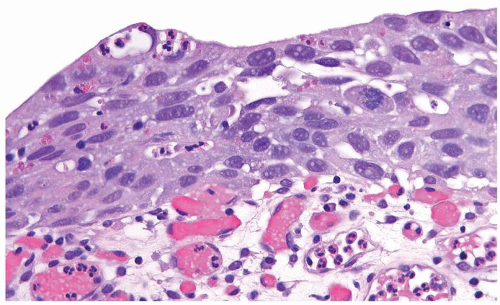 Figure 3.5.1 CIS with inflammation. Cells show marked nuclear pleomorphism. |
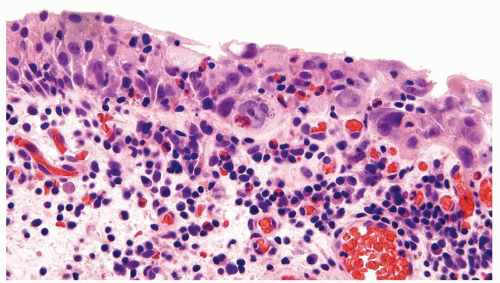 Figure 3.5.2 CIS with inflammation. Cells show marked nuclear pleomorphism. |
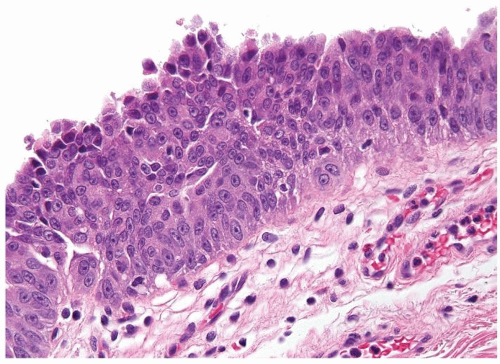 Figure 3.5.3 CIS with prominent nucleoli. In contrast to reactive changes, there is no inflammation in the urothelium, and nuclei are variable in size and shape. |
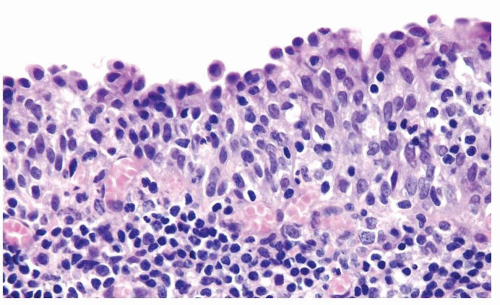 Figure 3.5.4 Reactive changes with numerous intramucosal lymphocytes and vesicular nuclei with visible nucleoli. |
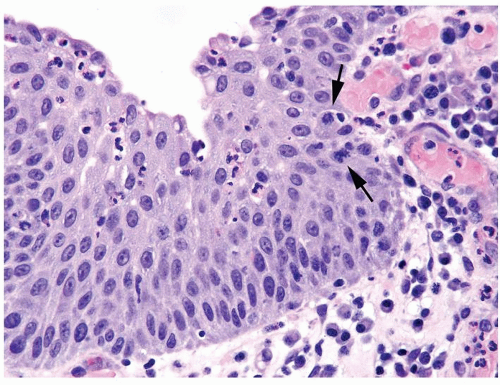 Figure 3.5.5 Reactive changes with numerous intramucosal neutrophils and vesicular nuclei with prominent nucleoli and mitotic figures (arrows). |
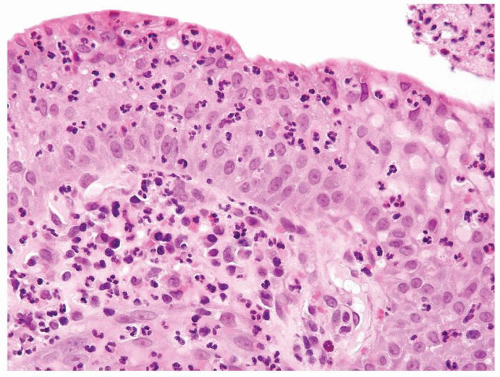 Figure 3.5.6 Reactive changes with numerous intramucosal neutrophils and vesicular nuclei with prominent nucleoli. Nuclei are uniformly enlarged and lack variation in shape. |
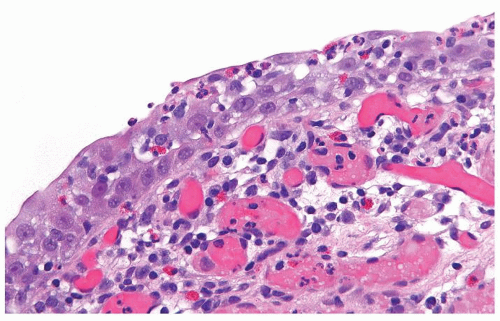 Figure 3.5.7 Reactive changes with numerous intramucosal neutrophils and eosinophils. Nuclei are vesicular with prominent nucleoli and are uniformly enlarged without pleomorphism. |
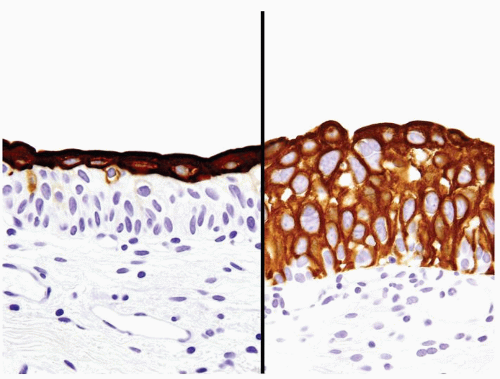 Figure 3.5.8 CK20 typically stains umbrella cells only in the normal and reactive urothelium (left) with diffuse CK20 immunoreactivity in dysplasia and CIS (right). |
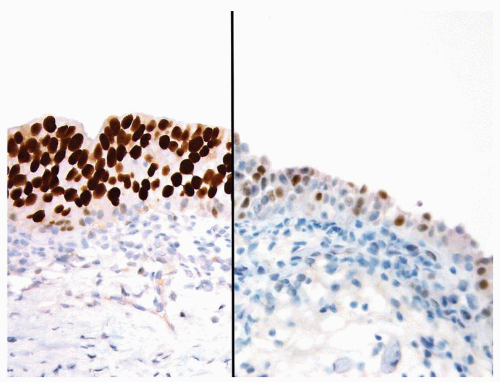 Figure 3.5.9 Diffuse strong p53 staining in CIS (left) compared to weak and moderate patchy p53 labeling (right) that is not diagnostic for CIS. |
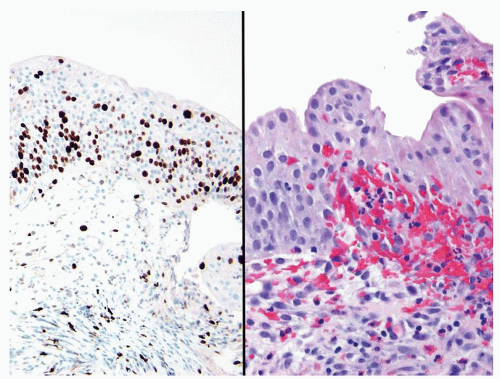 Figure 3.5.10 Reactive urothelium (right) with a marked increase in Ki-67 labeling (left). |
|
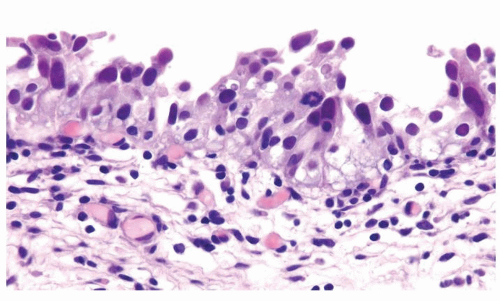 Figure 3.6.1 CIS with markedly enlarged hyperchromatic nuclei and mitotic figures and modest amount of cytoplasm. |
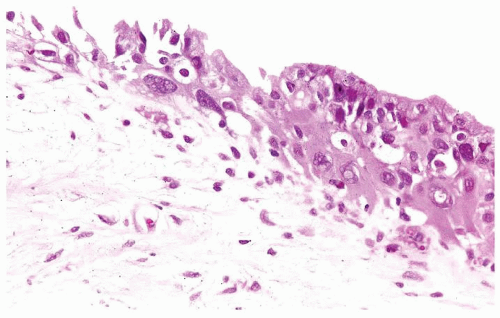 Figure 3.6.2 Radiation atypia with enlarged nuclei with a degenerative appearance with nuclear vesicles. Cells also have abundant spindled cytoplasm. |
 Figure 3.6.3 Radiation atypia with degenerative nuclear atypia and abundant cytoplasm. |
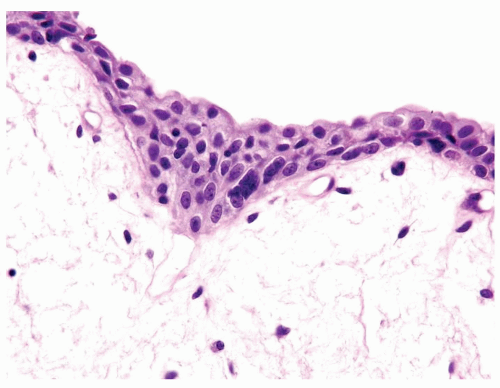 Figure 3.6.4 Radiation atypia with a multinucleated hyperchromatic nucleus. |
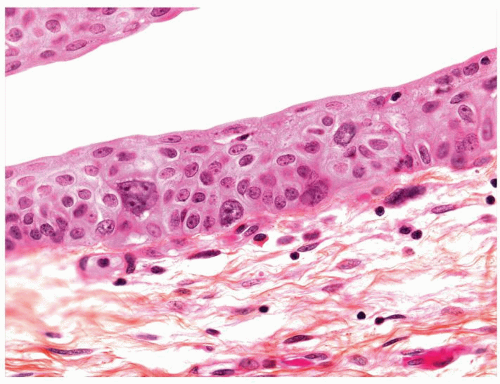 Figure 3.6.5 Radiation atypia with a multinucleated nucleus. |
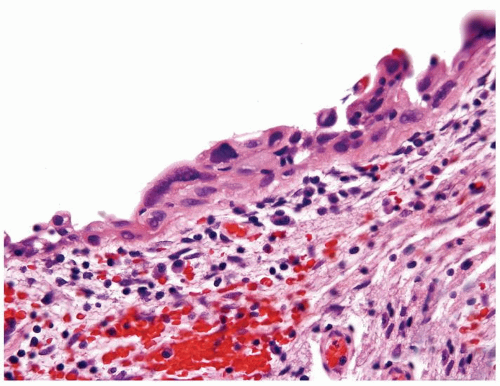 Figure 3.6.6 Radiation atypia with degenerative nuclear atypia and abundant cytoplasm. |
|
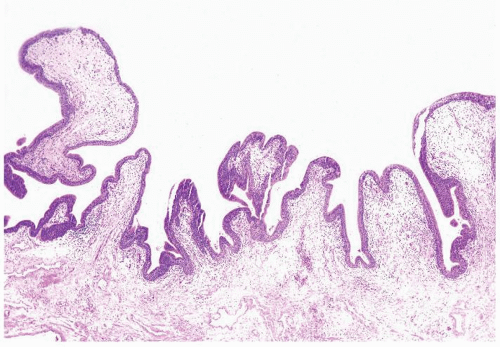 Figure 3.7.1 Polypoid cystitis with simple folds of pale, edematous urothelium. |
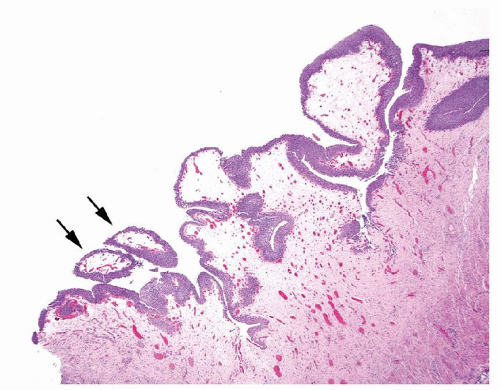 Figure 3.7.2 Polypoid cystitis with mostly simple folds with wide base but occasional smaller edematous papillary structures (arrows) that could be misdiagnosed as a papillary urothelial neoplasm. |
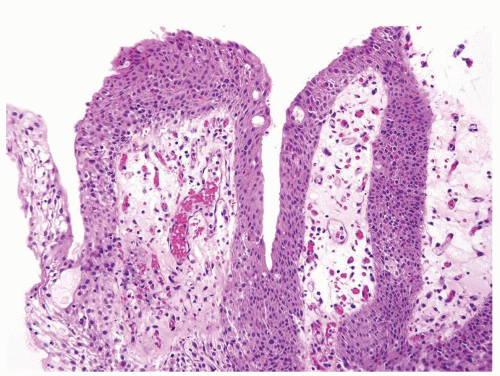 Figure 3.7.3 Polypoid cystitis with simple folds of pale edematous urothelium containing inflammatory cells. |
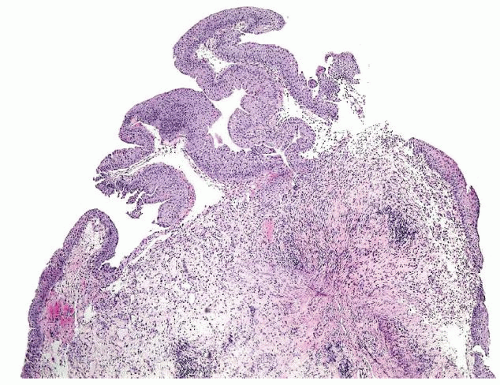 Figure 3.7.4 Polypoid cystitis with simple folds and densely fibrotic and inflamed stroma. |
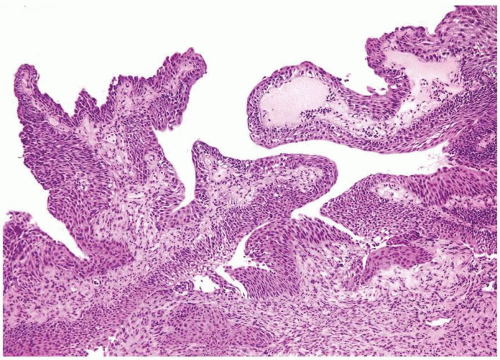 Figure 3.7.5 Polypoid cystitis with occasional branching folds and densely fibrotic and inflamed stroma. |
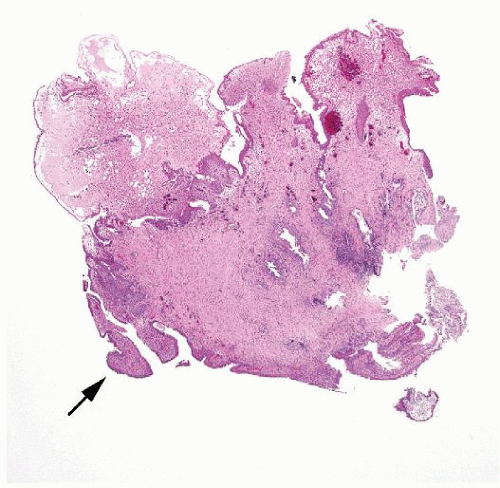 Figure 3.7.6 Typical polypoid cystitis (top) with simple broad based folds replaced by densely eosinophilic fibrotic stroma. Focal small fronds with fibrous cores (arrow) were misdiagnosed as papillary urothelial carcinoma. |
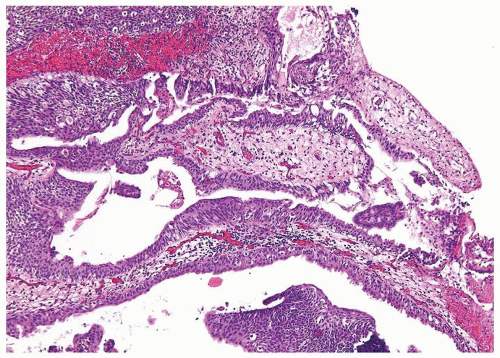 Figure 3.7.7 Unusual case of polypoid cystitis with long simple folds containing abundant inflammation and fibrous tissue. |
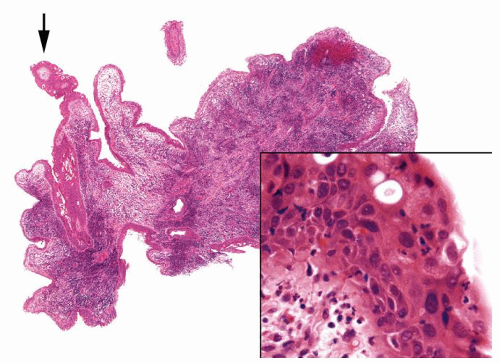 Figure 3.7.8 Polypoid cystitis with areas showing simple broad based folds with intense inflammation. Focal small fronds (arrow) were misdiagnosed as papillary urothelial carcinoma. Inset shows an inflamed reactive urothelium. |
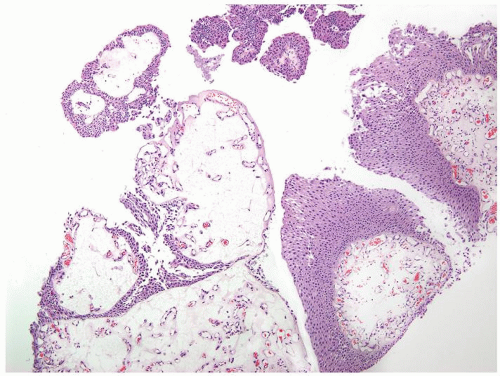 Figure 3.7.9 Low-grade papillary urothelial carcinoma with edematous yet not inflamed stalks containing numerous prominent capillaries. Focally, the urothelium is markedly thickened. |
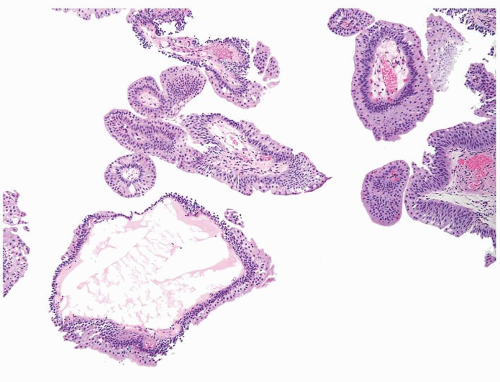 Figure 3.7.10 Low-grade papillary urothelial carcinoma with dilated lymphatic in stalk. Lesion has multiple “free-floating” fronds indicative of a complex branching papillary lesion. |
|
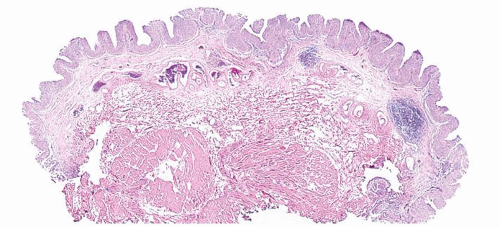 Figure 3.8.1 Papillary urothelial hyperplasia with thickened folds of the urothelium. |
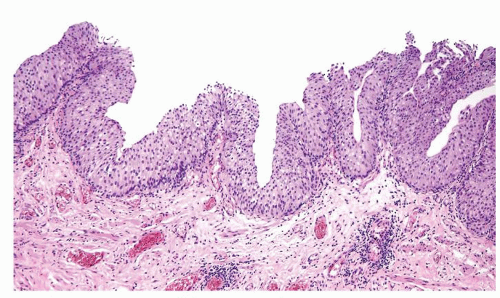 Figure 3.8.2 Papillary urothelial hyperplasia with thickened folds of the urothelium. |
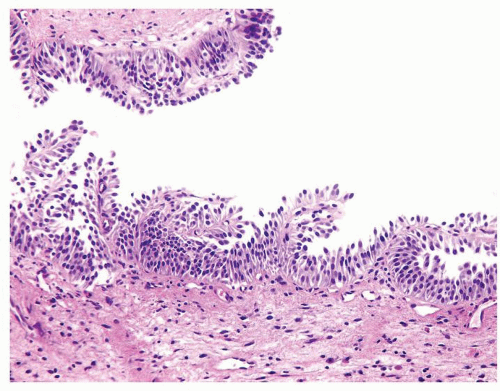 Figure 3.8.3 Papillary lesion that is borderline between papillary urothelial hyperplasia and early papilloma. |
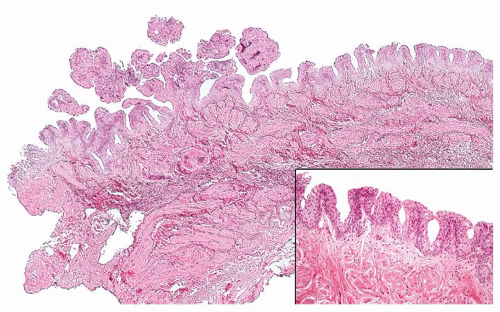 Figure 3.8.4 Papillary urothelial hyperplasia (right and inset) with adjacent papilloma (left). |
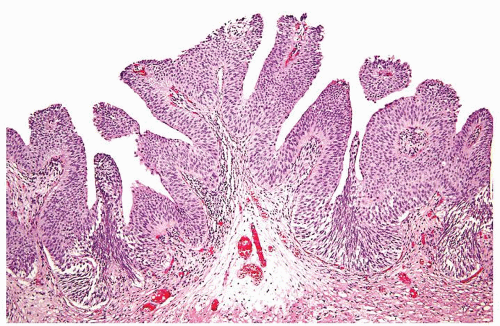 Figure 3.8.5 Early papilloma with branching and beginning of “detached” papillary fronds. |
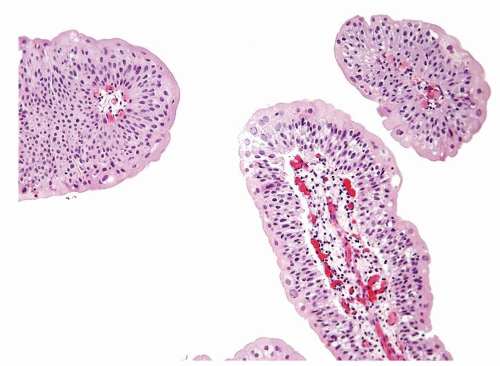 Figure 3.8.6 Papilloma with “free-floating” fronds. |
|
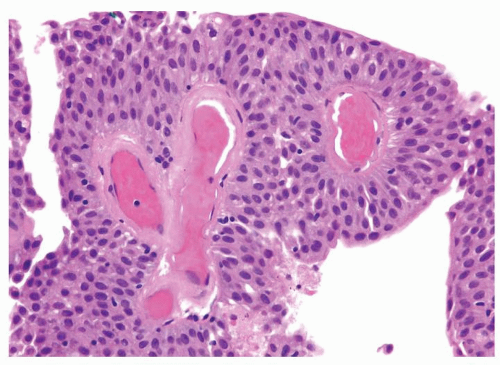 Figure 3.9.1 Papilloma with the urothelium of normal thickness and cytology. |
 Figure 3.9.2 Papilloma. |
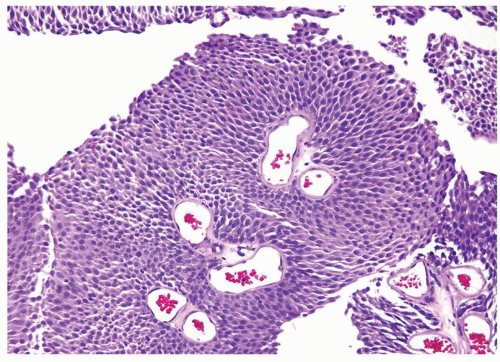 Figure 3.9.3 PUNLMP with the overtly thickened urothelium. |
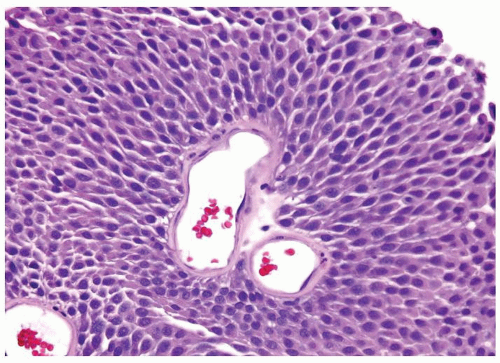 Figure 3.9.4 Same case as Figure 3.9.3 with benign cytology. |
|
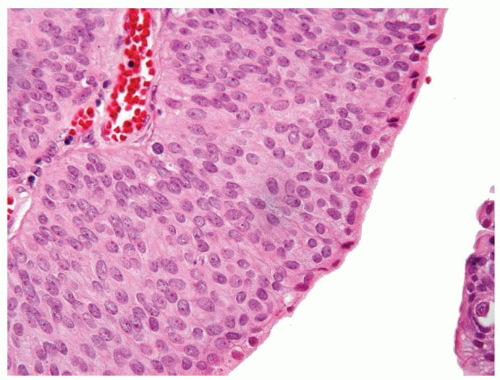 Figure 3.10.1 PUNLMP with uniform cytology, lacking scattered cells with nuclear hyperchromasia. |
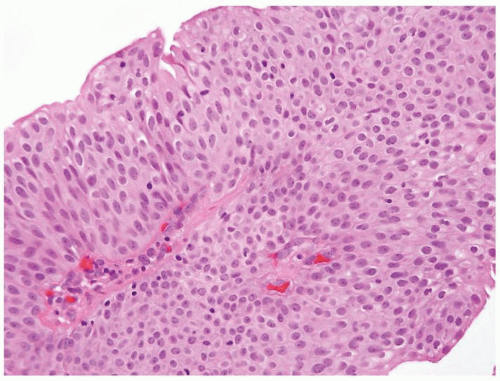 Figure 3.10.2 PUNLMP. |
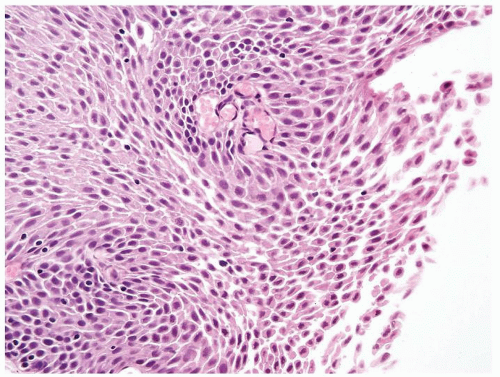 Figure 3.10.3 PUNLMP. |
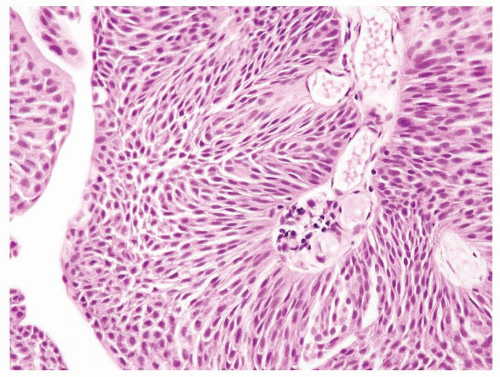 Figure 3.10.4 PUNLMP. |
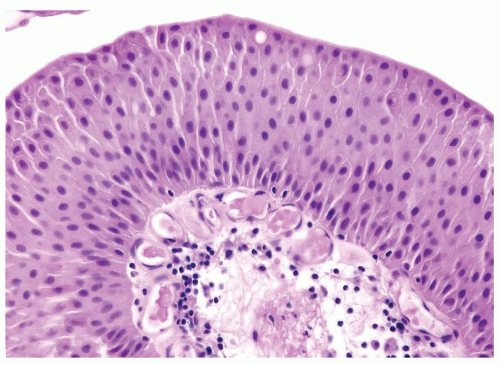 Figure 3.10.5 Low-grade papillary urothelial carcinoma with scattered hyperchromatic nuclei. |
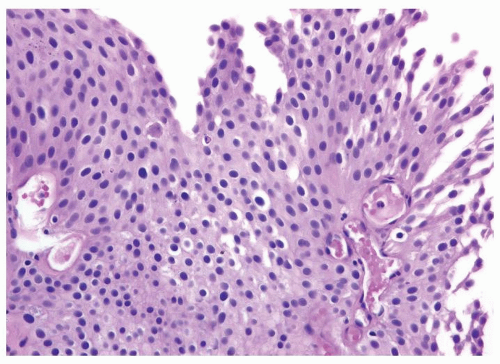 Figure 3.10.6 Low-grade papillary urothelial carcinoma with scattered hyperchromatic nuclei. |
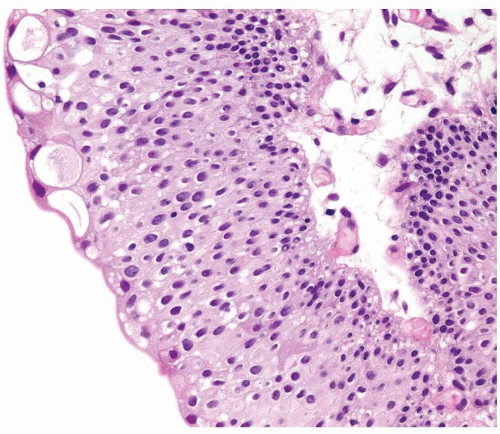 Figure 3.10.7 Low-grade papillary urothelial carcinoma with scattered hyperchromatic nuclei. |
 Figure 3.10.8 Low-grade papillary urothelial carcinoma with scattered hyperchromatic nuclei and mitotic figures (arrow). |
|
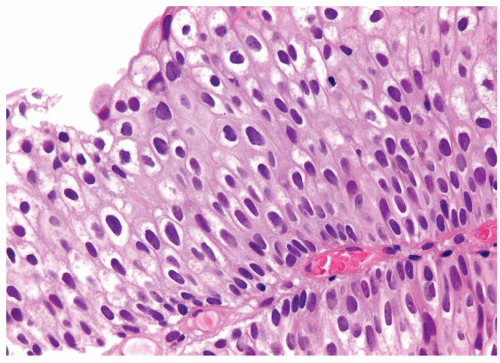 Figure 3.11.1 Low-grade papillary urothelial carcinoma with uniform polarity and scattered minimally enlarged hyperchromatic nuclei. |
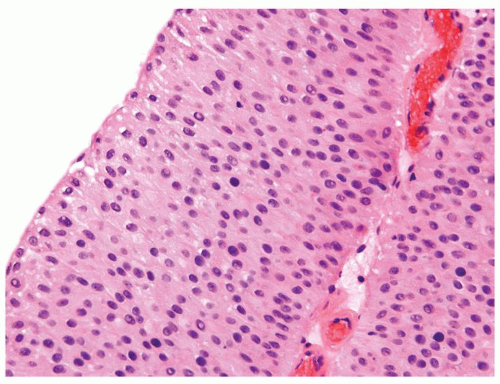 Figure 3.11.2 Low-grade papillary urothelial carcinoma with uniform polarity and scattered minimally enlarged hyperchromatic nuclei. |
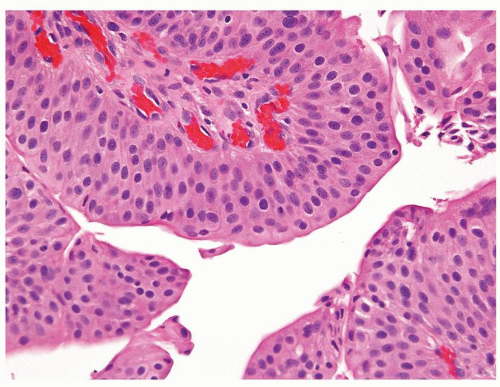 Figure 3.11.3 Low-grade papillary urothelial carcinoma with uniform polarity and scattered minimally enlarged hyperchromatic nuclei. |
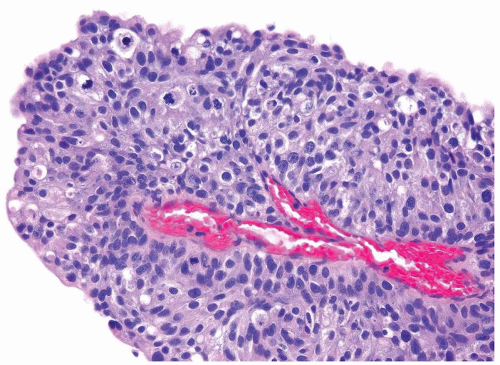 Figure 3.11.4 High-grade papillary urothelial carcinoma with loss of polarity with nuclei not lining up in uniform spatial arrangement. Numerous mitotic figures noted. |
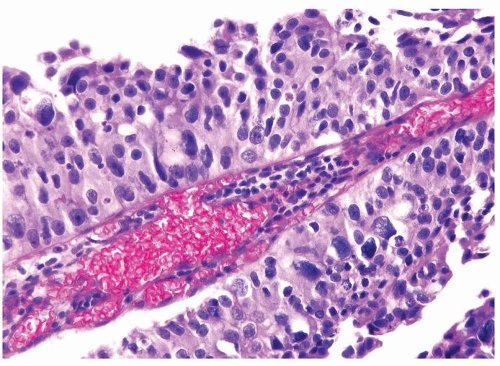 Figure 3.11.5 High-grade papillary urothelial carcinoma with marked pleomorphism. |
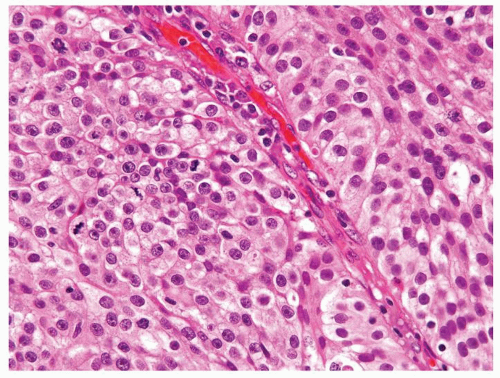 Figure 3.11.6 High-grade papillary urothelial carcinoma with diffuse prominent nucleoli and numerous mitotic figures. |
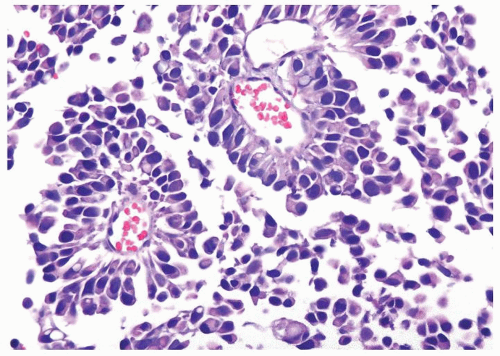 Figure 3.11.7 High-grade papillary urothelial carcinoma with dyscohesive cells with hyperchromatic nuclei. |
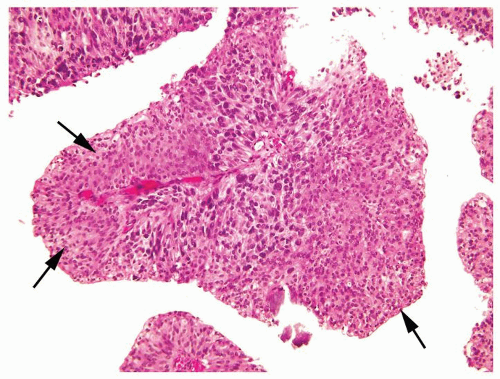 Figure 3.11.8 High-grade papillary carcinoma with areas showing more uniform cytology and preserved polarity (arrows) with rest of the tumor high grade. |
|
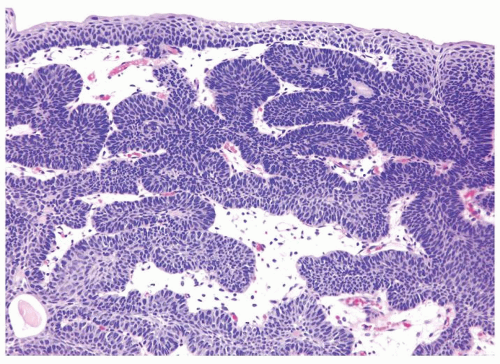 Figure 3.12.1 Inverted papilloma with anastomosing columns of the urothelium beneath the smooth surface. |
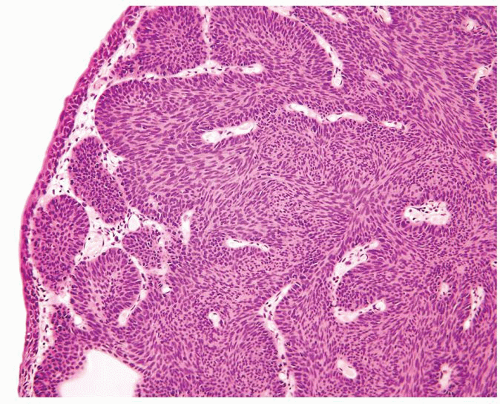 Figure 3.12.2 Inverted papilloma with anastomosing columns of the urothelium beneath the smooth surface. |
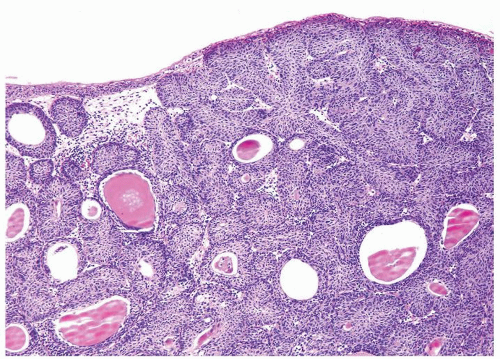 Figure 3.12.3 Inverted papilloma with colloid-filled cysts. |
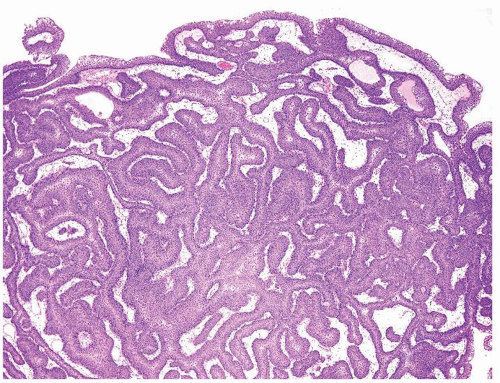 Figure 3.12.4 Inverted papilloma with anastomosing columns of the urothelium beneath the slightly polypoid surface. Rare fronds (left) in the setting of typical inverted papilloma do not change the diagnosis. |
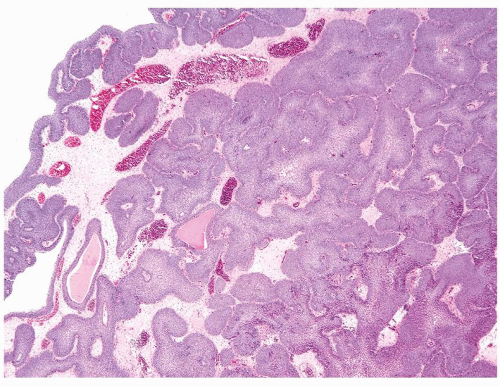 Figure 3.12.5 Typical inverted papilloma. |
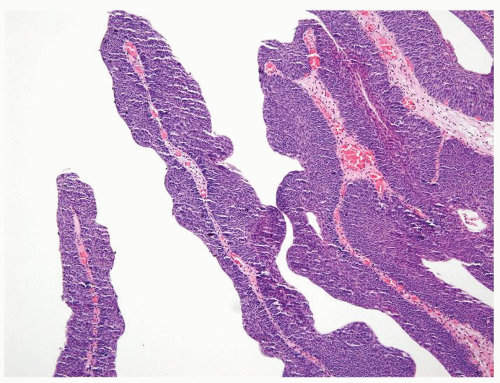 Figure 3.12.6 Same case as Figure 3.12.5 with focal papillary fronds. |
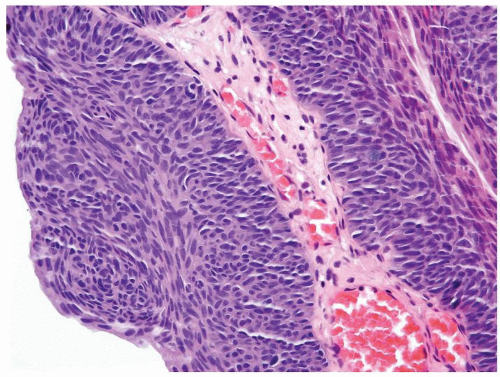 Figure 3.12.7 Higher magnification of Figure 3.12.6 with papillary fronds having the same spindled urothelium seen in the inverted portion of the tumor, still consistent with inverted papilloma. |
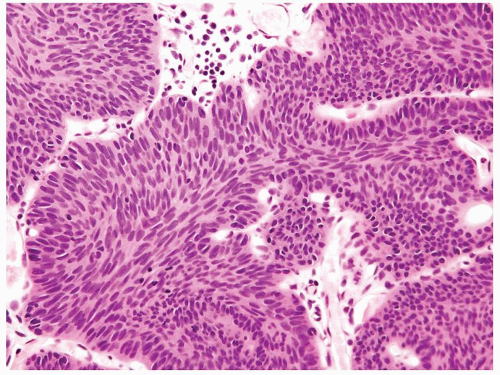 Figure 3.12.8 Inverted papilloma with streaming of nuclei parallel to columns. |
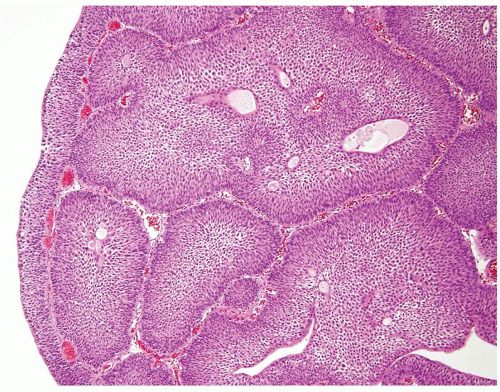 Figure 3.12.9 Inverted growth of PUNLMP with large rounded nests. |
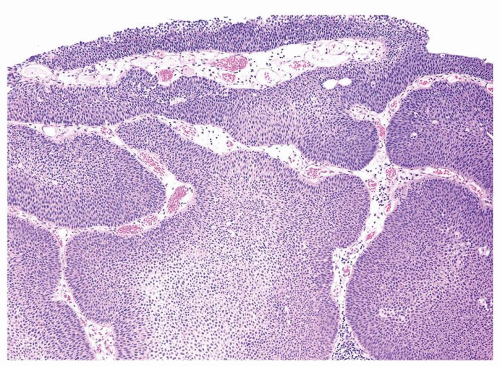 Figure 3.12.10 Inverted growth of low-grade papillary urothelial carcinoma with large rounded nests. |
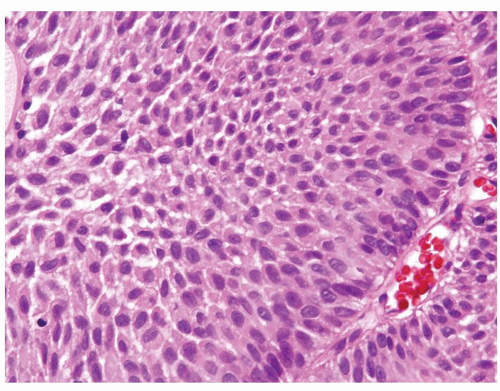 Figure 3.12.11 Same case as Figure 3.12.9 with bland cytology. |
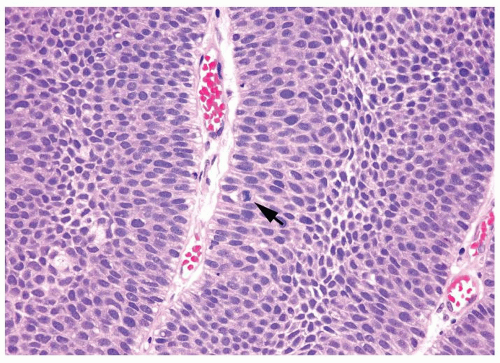 Figure 3.12.12 Same case as Figure 3.12.10 with scattered hyperchromatic nuclei and mitotic figures (arrow). |
|
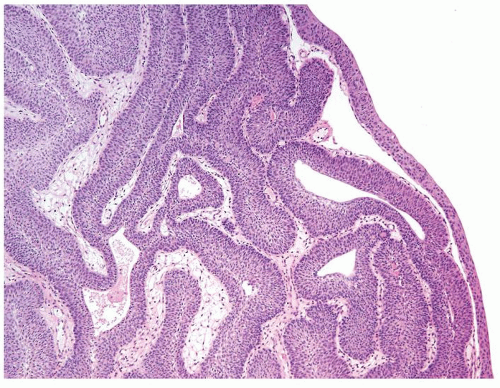 Figure 3.13.1 Inverted papilloma with smooth surface and underlying anastomosing thin columns of urothelium. |
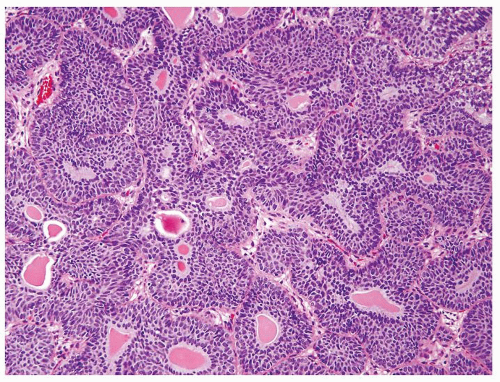 Figure 3.13.2 Inverted papilloma with anastomosing thin columns of urothelium with colloid cysts. |
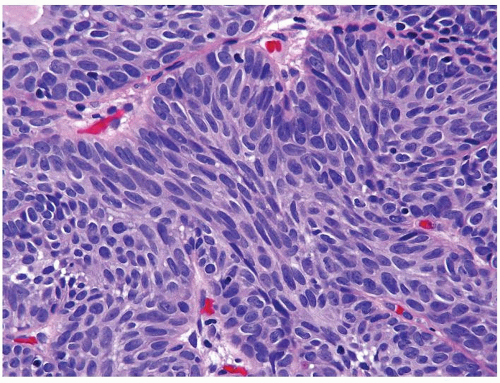 Figure 3.13.3 Inverted papilloma with streaming of nuclei parallel to columns and peripheral palisading of nuclei at epithelial-stromal interface. |
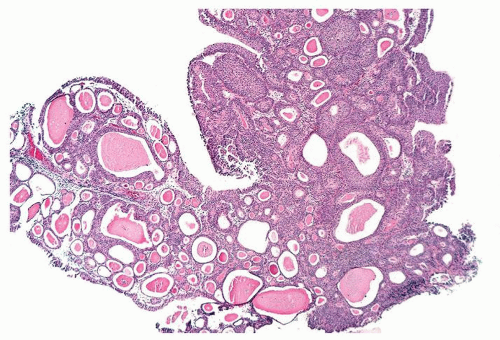 Figure 3.13.4 Polypoid florid proliferation of von Brunn nests mimicking a tumor. |
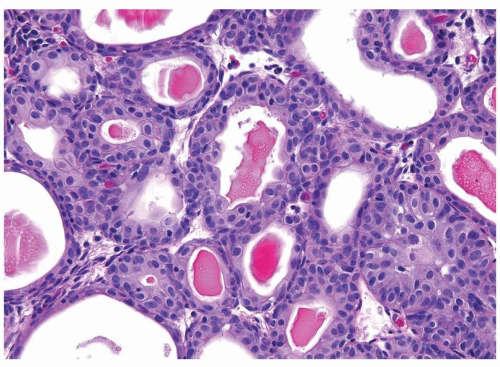 Figure 3.13.5 Same case as Figure 3.13.4 with rounded colloid-filled nests. |
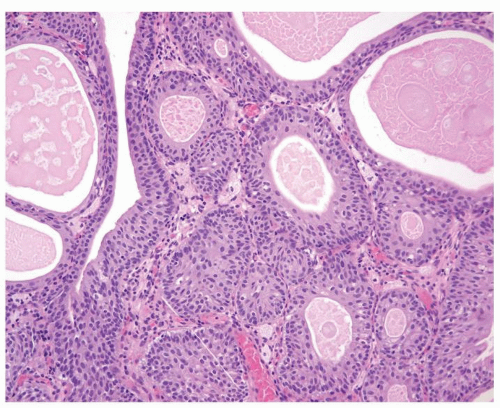 Figure 3.13.6 Rounded von Brunn nests with colloid. |
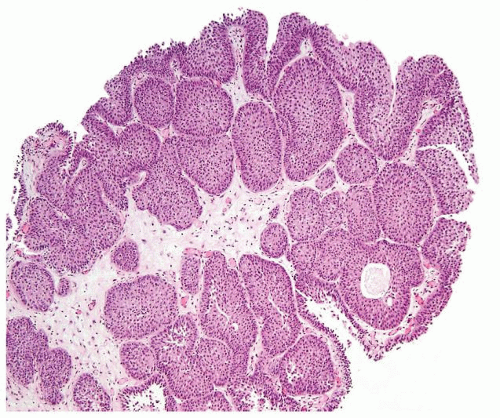 Figure 3.13.7 Florid proliferation of von Brunn nests resulting in a tumor-like lesion. |
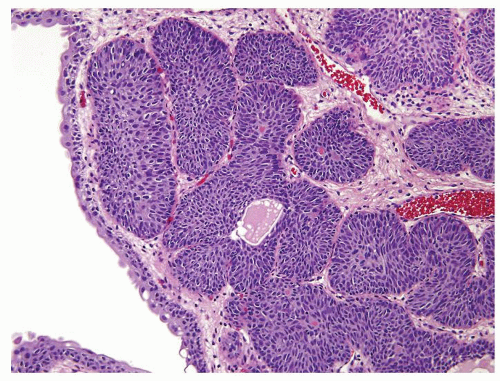 Figure 3.13.8 Proliferation of rounded von Brunn nests. |
|
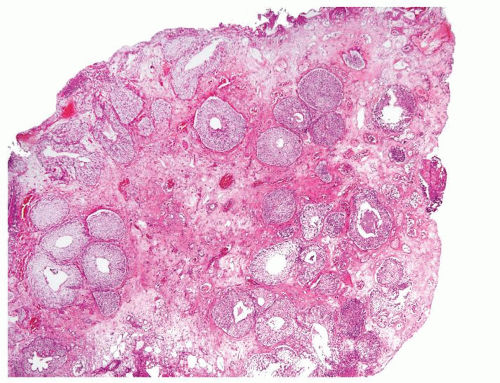 Figure 3.14.1 Proliferation of von Brunn nests in the bladder consisting of large uniform nests with central cyst formation. |
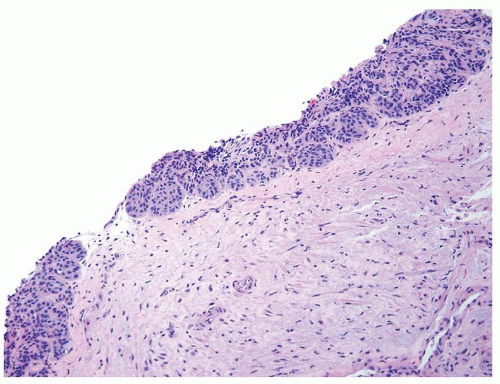 Figure 3.14.2 Proliferation of von Brunn nests in the bladder with small nests. The nests have a noninfiltrative base and cluster just beneath the surface. |
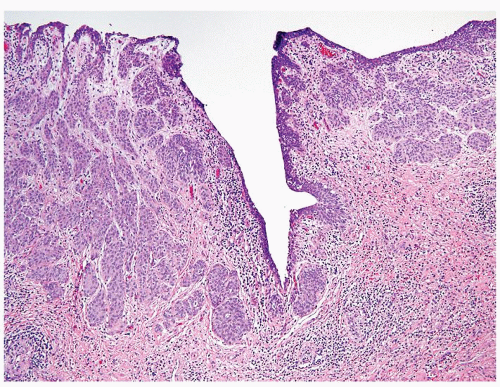 Figure 3.14.3 Proliferation of von Brunn nests in the bladder with small nests. The nests have a noninfiltrative base and cluster just beneath the surface. |
 Figure 3.14.4 Proliferation of von Brunn nests in the bladder with small nests arranged in a lobular and linear array beneath the urothelium. Nests are circumferential around the ureter and are noninfiltrative. |
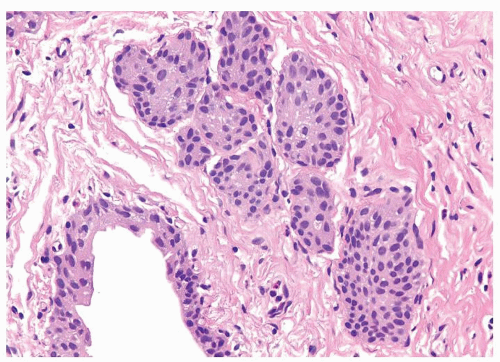 Figure 3.14.5 Same case as Figure 3.14.4 at higher magnification. |
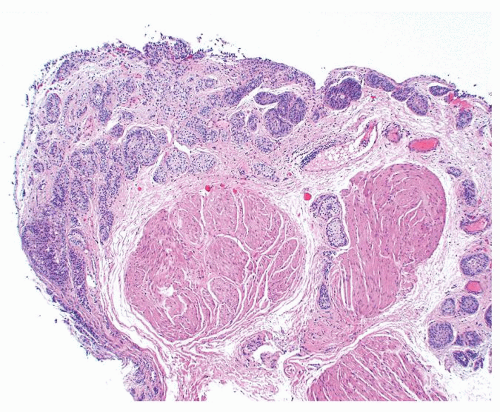 Figure 3.14.6 Nested carcinoma with smooth surface and small- and medium-sized nests infiltrating the muscularis propria. |
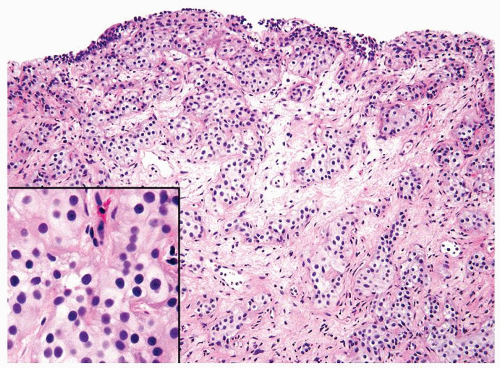 Figure 3.14.7 Nested carcinoma with smooth surface and small nests irregularly infiltrating lamina propria. Inset shows bland cytology. |
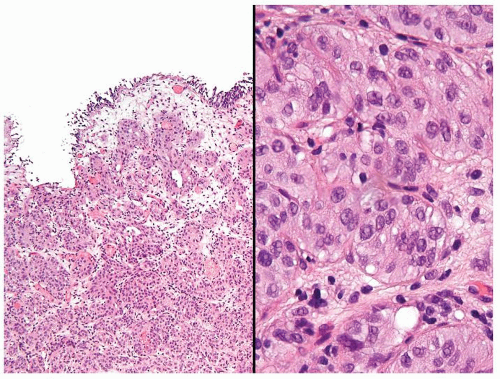 Figure 3.14.8 Nested carcinoma with crowded small nests filling the lamina propria (left) having minimal cytologic atypia (right). |
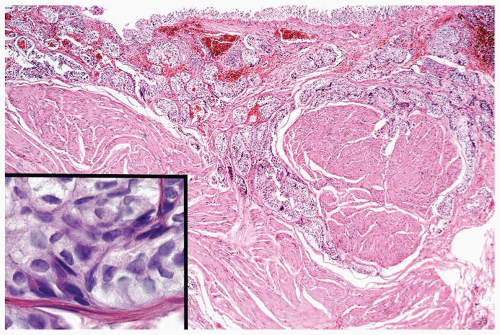 Figure 3.14.9 Nested carcinoma with irregular downward growth of small nests invading the muscularis propria. Inset shows no atypia. |
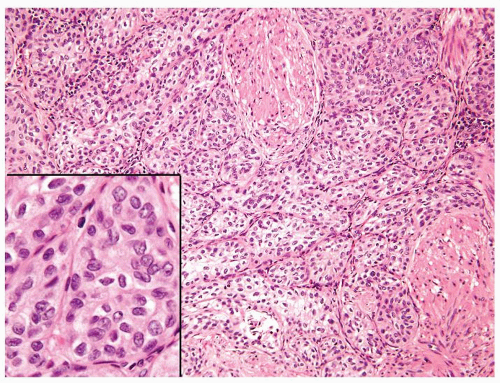 Figure 3.14.10 Nested carcinoma with back-to-back small nests invading the muscularis propria. Cells resemble normal urothelial cells with some even having nuclear grooves (inset). |
|
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


