Basal Cell Carcinoma
David Cassarino, MD, PhD
Key Facts
Terminology
Low-grade malignancy of basal keratinocytes
Etiology/Pathogenesis
Related to sun exposure, radiation, immunosuppression
May be derived from follicular stem cells
Clinical Issues
Very common: Most common cancer in humans
Prognosis usually excellent, most cases cured by excision
More aggressive subtypes, including infiltrative, micronodular, desmoplastic, and basosquamous, have higher rate of recurrence and low risk of metastasis
Treated by complete excision or electrodessication and curettage
Microscopic Pathology
Proliferation of nodules, nests, and cords of small basaloid cells with peripheral palisading, stromal retraction artifact, and mucinous material
Numerous mitotic and apoptotic figures typically present
Cells show enlarged hyperchromatic nuclei with inconspicuous nucleoli and scant amounts of eosinophilic cytoplasm
Top Differential Diagnoses
Squamous cell carcinoma
Actinic keratosis (on superficial shave biopsy)
Follicular neoplasms (trichoepithelioma and trichoblastoma)
Merkel cell carcinoma
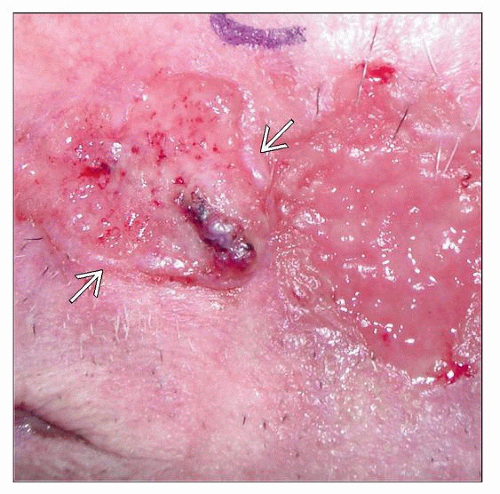 Clinical photograph of a large facial BCC shows areas of ulceration and granulation-like tissue surrounded by a raised border  . (Courtesy S. Yashar, MD.) . (Courtesy S. Yashar, MD.) |
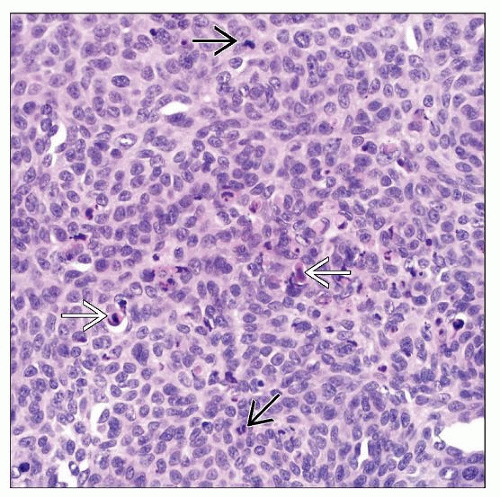 High magnification of a nodular BCC shows a sheet-like proliferation of atypical basaloid cells with high N:C ratios and numerous apoptotic  and mitotic figures and mitotic figures  . . |
TERMINOLOGY
Abbreviations
Basal cell carcinoma (BCC)
Synonyms
Basal cell epithelioma (BCE)
Trichoblastic carcinoma (not well accepted and should be discouraged)
Definitions
Low-grade malignancy of basaloid-appearing keratinocytes
ETIOLOGY/PATHOGENESIS
Multifactorial
Related to sun exposure (vast majority of cases)
Some cases may also be associated with radiation, immunosuppression (organ transplantation), burn scars
These cases tend to be more aggressive
May actually be derived from follicular stem cells (hence, “trichoblastic carcinoma”)
Genetics
Rare cases are associated with genetic syndromes including nevoid basal cell carcinoma (Gorlin) syndrome, xeroderma pigmentosum, basex syndrome, Rombo syndrome, and McKusick syndrome
Genes implicated include PTCH1 (Gorlin syndrome), P53, SOX9, BMI1, BAX, RMRP
CLINICAL ISSUES
Epidemiology
Incidence
Extremely common: Most common cancer in humans when skin cancers are included
Accounts for 70% of primary cutaneous malignancies
Age
Typically older adults; few cases in young adults
If in a child, should consider a genetic syndrome
Gender
Slightly greater incidence in males
Ethnicity
Caucasian/light-skinned individuals
Rare in darker skin types
Site
Most common in head and neck region (up to 80% of cases)
About 15% occur on trunk and shoulders
Very rare cases involve lips, breast, axillae, groin, inguinal region, and genitalia
Presentation
Typically papular, plaque-like, or nodular lesion
Often present as a pearly, translucent papule with telangiectasia
Larger lesions often ulcerated with bleeding &/or overlying crusting
Minority of cases are pigmented, more often in Asians and Africans
Treatment
Surgical approaches
Complete excision or electrodessication and curettage (ED&C)
Mohs micrographic surgery often used in facial cases
Prognosis
Usually excellent, cured by local excision
More aggressive subtypes, including micronodular, infiltrative, desmoplastic, and basosquamous, have higher rate of recurrence and increased risk of metastasis
Overall risk of metastasis estimated at 0.05%
MACROSCOPIC FEATURES
Size
Variable, small (few mm) to large (several cm)
MICROSCOPIC PATHOLOGY
Histologic Features
Tumor is composed of nodules, nests, &/or infiltrative cords
Overlying ulceration and serum crusting often present in large tumors
Proliferation of small basaloid cells with peripheral palisading
Stromal retraction artifact
Between tumor cells and stroma
Mucinous material may be present
Numerous mitotic and apoptotic figures present
Cells show enlarged hyperchromatic nuclei with inconspicuous or small nucleoli and scant eosinophilic cytoplasm
Variants
Superficial-multicentric: Superficial nests attached to epidermis separated by areas of uninvolved epidermis
Nodular: Large, rounded predominantly dermal-based nests with prominent peripheral palisading
Micronodular: Predominantly dermal-based infiltrative proliferation of small nests
Infiltrative: Small cords and nests, often deeply invasive
Desmoplastic/sclerosing/morpheaform: Infiltrative strands and nests associated with dense sclerotic stroma
Infundibulocystic: Mature folliculocystic spaces containing keratinous material
Basosquamous/metatypical: Prominent areas of squamous differentiation (may mimic squamous cell carcinoma [SCC]), less peripheral palisading present
Fibroepithelioma of Pinkus: Numerous small, anastomosing cords of basaloid cells attached to the epidermis
Rare variants include adenoid, clear cell, signet ring cell, plasmacytoid/myoepithelial, and BCC with neuroendocrine differentiation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


