Axillary Node Biopsy and Axillary Node Dissection
Laura A. Adam
Neal W. Wilkinson
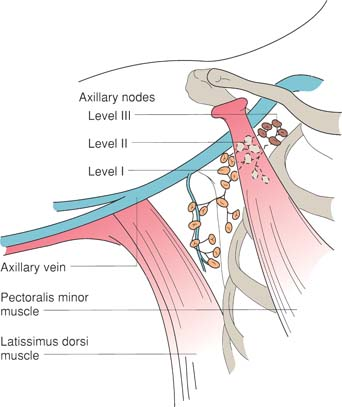
Axillary lymph node dissection typically refers to the more limited resection of topographic group I and group II axillary lymph nodes (orientation figure). It is most commonly performed for breast cancer, and may be performed in conjunction with mastectomy (termed a modified radical mastectomy; see Chapter 16) or as an isolated axillary node dissection with lumpectomy, as illustrated in this chapter. Often, a sentinel lymph node biopsy will have been performed previously, either as a separate surgical procedure or during the initial phase of the same operation.
Axillary node dissection may also be used for treatment of other malignancies (e.g., malignant melanoma). This chapter first discusses the technical modifications required when axillary node dissection is done alone. The final section of this chapter describes a more limited axillary node sampling procedure that is performed for staging of breast carcinomas. The aim of this more limited procedure is to remove a sampling of low axillary nodes. This procedure is rarely performed now, having been superseded by sentinel lymph node biopsy.
Steps in Procedure
Position patient supine, with arm extended on armboard
Transverse incision below hair-bearing area or oblique incision just behind lateral edge of pectoralis major muscle
Raise flaps
Identify lateral edge of pectoralis major muscle
Dissect under pectoralis major muscle, preserving median pectoral neurovascular bundle
Identify pectoralis minor muscle and dissect under it (sometimes, it may be divided or excised to facilitate dissection)
Identify axillary vein and trace it laterally
Identify long thoracic nerve and incise fascia lateral to it; mobilize the nerve medially
Identify thoracodorsal neurovascular bundle and preserve it
Sweep all fatty node-bearing tissue inferiorly and laterally, preserving nerves and axillary vein
Orient specimen
Obtain hemostasis and place closed suction drains
Close incision in layers
Axillary Sampling
Shorter but similar incision
Dissection is limited to level I and some level II nodes
Preserve nerves as noted above
Hallmark Anatomic Complications
Injury to median pectoral nerve
Injury to long thoracic nerve (winged scapula)
Injury to thoracodorsal nerve
Injury to axillary vein
Division or injury to intercostobrachial nerve
List of Structures
Pectoralis major muscle
Pectoralis minor muscle
Clavipectoral fascia
Lateral pectoral nerve
Medial pectoral nerve
Thoracodorsal nerve
Long thoracic nerve
Axillary artery
Axillary vein
Thoracoacromial artery
Thoracodorsal vein
 |
Axillary Node Dissection
Choice of Incision and Elevation of Flaps (Fig. 19.1)
Technical Points
Position the patient with the arm extended on an armboard with a bump under the shoulder if necessary (see Chapter 17). If sentinel node biopsy has been performed at an earlier time, plan an incision which excises and extends the previous scar. If sentinel node biopsy was done during the same operative procedure and returned positive, then extend the sentinel node incision in both directions.
In general, an oblique incision just lateral to the lateral border of the pectoralis major muscle provides excellent access to the axilla. Placing the incision just lateral to the muscle edge allows the scar to fall behind the muscle, where it is less noticeable. A more cosmetically appealing transverse or U-shaped incision may be used. This transverse incision should be planned to lie below the hair-bearing portion of the axilla. Patient habitus and location of sentinel lymph node may lead one incision or the other to be preferable in a specific situation. Create skin flaps to expose the subcutaneous tissues.
Anatomic Points
Discrete superficial and deep fascia is not encountered in the axilla. Instead, the axillary fascia (derived from the fascia of the pectoralis major, latissimus dorsi, and serratus anterior muscles as well as the fascia investing the muscles of the arm) is adherent to the superficial fascia and is, in the hollow of the armpit, along with the suspensory ligament of the axilla, a continuation of the clavipectoral fascia.
The axillary lymph nodes are predominantly located on the medial side of the axillary neurovascular bundle, and along the medial axillary wall. For convenience, these are described in five groups by anatomists. Terms in parentheses indicate the approximate equivalent in Haagensen’s system. The lateral group (axillary), on the third part of the axillary neurovascular bundle, drains the upper limb. The subscapular (scapular) or posterior group, located around the subscapular artery and vein, drains the shoulder and posterior thorax. The pectoral (external mammary) group, which is associated with the lateral thoracic
vessels along the inferolateral border of the pectoralis major muscle, drains and receives lymph from the anterior thoracic wall, including the lateral breast. These three groups drain into the central group of (central) lymph nodes, which is located approximately on the second part of the axillary neurovascular bundle. The apical group (subclavian), associated with the first part of the axillary neurovascular bundle, receives lymphatics from the central group as well as from the upper outer quadrant of the mammary gland.
vessels along the inferolateral border of the pectoralis major muscle, drains and receives lymph from the anterior thoracic wall, including the lateral breast. These three groups drain into the central group of (central) lymph nodes, which is located approximately on the second part of the axillary neurovascular bundle. The apical group (subclavian), associated with the first part of the axillary neurovascular bundle, receives lymphatics from the central group as well as from the upper outer quadrant of the mammary gland.
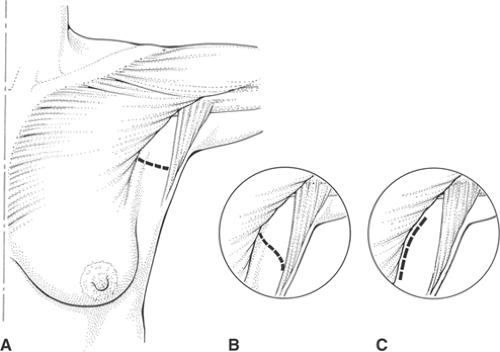 Figure 19-1 Choice of Incision and Elevation of Flaps (From Dixon JM, Soon PSH. Breast-conserving surgery. In: Fischer JE, Bland KI, eds. Mastery of Surgery. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.) |
Surgeons commonly use a different terminology (topographic) for axillary lymph nodes. Topographic group I nodes include the pectoral, subscapular, and lateral nodes. These are the nodes lateral to the pectoralis minor muscle. Topographic group II nodes are under the pectoralis minor muscle and correspond to the central nodes, whereas topographic group III nodes are medial to the pectoralis minor muscle and correspond to the apical nodes (see orientation figure).
Exposure of Nerves and Axillary Vein (Fig. 19.2)
Technical Points
If a sentinel node biopsy has been done, avoid the temptation to reenter the sentinel node cavity. Instead, work through clean tissue planes and excise this cavity with the specimen. First,
identify the lateral border of the pectoralis major muscle and clean the fatty tissue from the underside of the muscle (Fig. 19.2A, B). Take care to preserve the neurovascular bundle to the pectoralis major muscle. This bundle comes from above, and will generally retract medially and cephalad out of the field if gently displaced. Place a retractor under pectoralis major muscle. Identify the pectoralis minor muscle and incise the clavipectoral fascia on each side of this muscle. Divide the pectoralis minor muscle (if necessary) to gain access to the axillary vein. Dissect medially in the anterior adventitial plane of the vein to the surgical apex of the axilla. Follow the axillary vein laterally, dividing any small vessels that cross over the vein. The general rule is that any structure that crosses the axillary vein is safe to take, as is any structure that terminates in the vein.
identify the lateral border of the pectoralis major muscle and clean the fatty tissue from the underside of the muscle (Fig. 19.2A, B). Take care to preserve the neurovascular bundle to the pectoralis major muscle. This bundle comes from above, and will generally retract medially and cephalad out of the field if gently displaced. Place a retractor under pectoralis major muscle. Identify the pectoralis minor muscle and incise the clavipectoral fascia on each side of this muscle. Divide the pectoralis minor muscle (if necessary) to gain access to the axillary vein. Dissect medially in the anterior adventitial plane of the vein to the surgical apex of the axilla. Follow the axillary vein laterally, dividing any small vessels that cross over the vein. The general rule is that any structure that crosses the axillary vein is safe to take, as is any structure that terminates in the vein.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


