Aneurysmal Bone Cyst
Jessica M. Comstock, MD
Key Facts
Terminology
Solitary expansile lesion, most commonly involving long bones or spine
Clinical Issues
1st and 2nd decade of life
Secondary reactive lesion in many cases
Can coexist with many tumors
Benign but locally aggressive
Image Findings
Can look malignant
Microscopic Pathology
Always look for secondary tumors
Blood-filled cystic spaces
Fibrous septa separate cystic spaces
Septae contain spindle cells, giant cells, hemosiderin, osteoid
Most ABCs have some solid areas
Solid ABC/giant cell reparative granuloma
Most common in mandible, maxilla, and small bones of hands and feet
2nd to 3rd decade of life
No cystic cavities grossly or microscopically
Ancillary Tests
17p13 rearrangement is characteristic
Top Differential Diagnoses
Giant cell tumor
Telangiectatic osteosarcoma
Simple bone cyst
Low-grade osteosarcoma
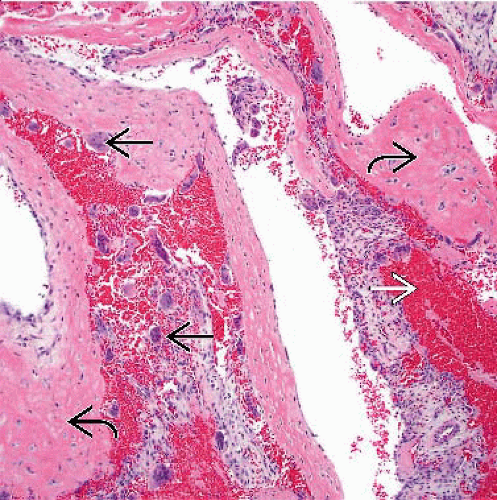 The characteristic features of aneurysmal bone cyst include hemorrhage  , giant cells , giant cells  , and thin osteoid , and thin osteoid  . . |
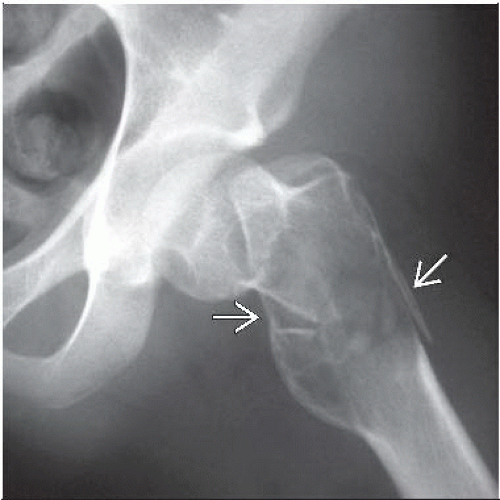 Anteroposterior radiograph shows a lytic expansile lesion in the proximal femoral metaphysis with pathologic fracture  . . |
TERMINOLOGY
Abbreviations
Aneurysmal bone cyst (ABC)
Definitions
Solitary expansile lesion, most commonly involving long bones or spine
ETIOLOGY/PATHOGENESIS
Developmental Anomaly
Proposed etiology for secondary ABCs implicates venous obstruction or arteriovenous fistula formation after bone trauma
Chromosomal abnormalities in primary ABCs indicate clonal tumor
CLINICAL ISSUES
Epidemiology
Age
1st and 2nd decade of life
Usually before skeletal maturity
Gender
Slightly more common in females
Site
Metaphysis of long bones
Eccentric
Dorsal elements of spine
Not seen in coccyx
Can affect multiple vertebrae
Cord compression is common
Presentation
Pain, tenderness
Swelling
Natural History
ABC is secondary reactive lesion in many cases
Can coexist with many tumors, such as
Osteoblastoma
Chondroblastoma
Nonossifying fibroma
Fibrous dysplasia
Treatment
Surgical approaches
Curettage
Prognosis
Benign but locally aggressive
Commonly recurs after curettage



