Adrenalectomy: Open Posterior
Barbra S. Miller
DEFINITION
Adrenal masses may be benign or malignant and functional or nonfunctional with regard to excess hormone secretion. An open posterior approach should be considered if:
An anterior, lateral, or posterior retroperitoneoscopic approach is not feasible in a patient with a benign or metastatic adrenal tumor.
An open anterior approach is not feasible in patients who have undergone previous extensive upper abdominal surgery and are presumed to have dense adhesions limiting access.
Conversion from a retroperitoneoscopic posterior approach to an open approach is required.
Both adrenals need to be removed and repositioning of the patient during the case is to be avoided.
DIFFERENTIAL DIAGNOSIS
Primary adrenal adenoma
Primary adrenocortical carcinoma
Cyst
Metastatic cancer
Pheochromocytoma
Ganglioneuroma
Adjacent paraganglioma
Soft tissue tumor
PATIENT HISTORY AND PHYSICAL FINDINGS
All adrenal abnormalities should be evaluated in a systematic fashion, including a thorough history and physical examination investigating the possibility of a hormone-secreting mass. This includes the possibility of a pheochromocytoma, Cushing’s syndrome, primary hyperaldosteronism, and hypertestosteronemia. Specifically, the patient should be questioned regarding poorly controlled hypertension, diabetes, edema, diaphoresis, tachycardia, palpitations, sudden severe headaches, flushing, and easy bruising. The physical exam should look for evidence of central obesity, edema, peripheral wasting, core muscle weakness, a buffalo hump, striae, thin skin, and facial plethora. Because the adrenal gland is situated in the retroperitoneum, unless it is extremely large, palpation of the mass is usually unable to be achieved.
IMAGING AND OTHER DIAGNOSTIC STUDIES
All adrenal masses should undergo appropriate biochemical testing. Even in the absence of signs or symptoms, patients should have at a minimum: potassium, aldosterone, renin, plasma fractionated metanephrines (followed by 24-hour urine metanephrines and normetanephrines, catecholamines, and vanillylmandelic acid (VMA) if plasma values are abnormal), 24-hour urine-free cortisol, and adrenocorticotropic hormone (ACTH). Some physicians may also perform a low-dose dexamethasone suppression test and obtain dehydroepiandrosterone Sulfate (DHEA-S) and free testosterone, among other laboratory tests.
Imaging studies should include an adrenal protocol computed tomography (CT) scan (to assess imaging characteristics and calculate washout percentage of contrast from the tumor) or magnetic resonance imaging (MRI) (to assess decrease in signal between in and out of phase images) and 18F-Fluorodeoxyglucose (18FDG) positron emission tomography (PET) CT if malignancy is questioned (FIG 1).
Additional imaging studies may be required depending on the functionality of the tumor (metaiodobenzylguanidine [MIBG] for some pheochromocytoma patients, adrenal vein sampling for hyperaldosteronism, etc.).
Fine needle aspiration or core biopsy is not recommended if adrenocortical carcinoma is questioned. FNA may be useful if metastasis to the adrenal gland is in the differential and the adrenal tumor is the most accessible site of metastasis in the setting of multiple sites of metastatic disease. If biopsy is performed, it is imperative to first biochemically rule out pheochromocytoma.
SURGICAL MANAGEMENT
Adrenal tumors, if benign appearing by imaging criteria, nonfunctional, and therefore not requiring resection, should be reevaluated with at least one additional CT scan or MRI 6 to 12 months after the initial imaging study to ensure stability in size and internal imaging characteristics. Some advocate for a longer period of follow-up imaging for 2 years with reevaluation of biochemistry for 4 years.1
Functional tumors leading to hormone excess, indeterminate masses, and those suspected of being adrenocortical carcinoma or isolated metastatic disease from another primary tumor without evidence of widespread metastatic disease should be removed.
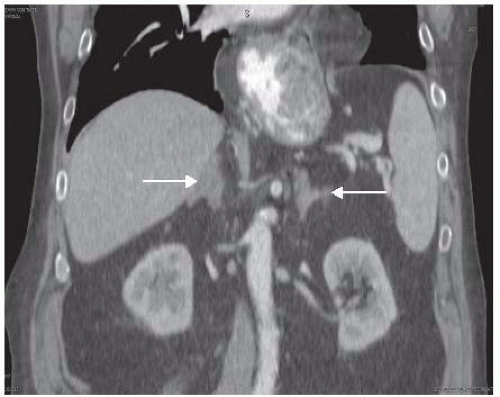 FIG 1 • Bilateral hyperplastic adrenal glands (arrows) with benign imaging characteristics are shown in an obese patient with Cushing’s disease requiring bilateral adrenalectomy. |
Preoperative Planning
The surgeon must evaluate available imaging studies for possible adrenocortical carcinoma or tumor involvement of adjacent organs, vessels, and lymphadenopathy. An open posterior approach is not optimal for removing adrenocortical carcinomas or large tumors, as the working space is limited by the rib cage and does not allow for multivisceral resections. These types of tumors should be approached by an open anterior or thoracoabdominal approach.
The surgeon should evaluate the position of the adrenal gland with respect to the overlying rib that will need to be resected as well as any visible vasculature supplying or draining the adrenal gland.
The risks, benefits, and alternatives to surgery are discussed with the patient including potential need for steroid supplementation in the postoperative setting. Patients with pheochromocytomas should be adequately alpha blocked and volume replete. Beta blockade may also be necessary. A potassium level should be checked the morning of surgery and treated as necessary in patients with Conn’s syndrome (hyperaldosteronism).
Routine prophylactic antibiotics and deep vein thrombosis (DVT) prophylaxis are administered prior to surgery, and sequential compression devices are applied.
A general endotracheal anesthetic is administered.
Common to all approaches, skin preparation with clipping rather than shaving is prepared, and the surgical area is prepped and draped in a sterile fashion.
Positioning
Patients are intubated and a Foley catheter is placed prior to placing the patient in a modified prone position. Several methods for positioning may be used, including use of the Wilson frame, the Cloward surgical saddle, gel rolls, and flexion of the table (FIG 2). All of these have the common goal of creating a gentle flexion of the spine. Space is also created for the abdominal contents to shift away from the retroperitoneum.
All pressure points are padded appropriately.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


