Key Points
Disease summary:
Gallstone disease is a complex trait resulting from an interaction between genetic predisposition and environmental risk factors. In patients carrying rare monogenic mutations gallstones develop mostly due to genetic risk factors. On the other hand, in carriers of common risk variants, stones form predominantly due to environmental triggers interacting with these genetic variants.
Gallstone disease affects 10% to 50% of adults in developed countries; prevalence rates of gallstones in developing countries are rising constantly. The disease is rare in children.
Gallstones can be divided into three subtypes: cholesterol gallstones, which are most common (>95%) and compromise predominantly cholesterol, pigment gallstones that mainly consist of calcium bilirubinate, and mixed stones.
Nongenetic risk factors include age, parity, metabolic syndrome, obesity, and insulin resistance.
Most patients with gallstones remain asymptomatic throughout their lives; biliary colic represents the most common sign of symptomatic disease, which develops in 20% of patients.
In symptomatic patients early surgery is indicated due to recurrence of symptoms and high complication rates.
Differential diagnosis:
Abdominal aneurysm, acute and chronic pancreatitis, biliary dyskinesia, diverticulitis, functional gastrointestinal disorders, peptic ulcer disease
Monogenic forms:
Monogenic cholelithiasis is rare but the presence of predisposing variants substantially increases the risk of disease and the recurrence of stones after treatment. Bilirubin gallstones can be caused by single-gene mutations known to increase the risk of hemolytic anemias, in particular in children (hereditary spherocytosis: ANK1, EPB42, SLC4A1, SPTA1, SPTB; sickle cell disease: HBB; thalassemia major and intermedia: HBB; erythrocyte enzyme deficiencies: AKI, G6PD, GPI, GSR, PGK1, PKLR, TPII). Patients with risk variants of ABCB4, the gene encoding the hepatobiliary phosphatidylcholine floppase, develop the so-called low phospholipid-associated cholelithiasis (LPAC) syndrome.
Family history:
Gallstone disease develops up to five times more frequently in family members of affected individuals.
Twin studies:
Twin studies have demonstrated that in Europeans the genetic risk factors account for approximately 25% of total disease risk.
Environmental factors:
Environmental effects account for 75% of gallstone risk.
Genome-wide association scans (GWASs):
To date, one GWAS on gallstones has been published. The analysis of 280 cases and 360 controls in the screening panel, subsequently replicated in 1832 German and 167 Chilean patients, identified a common variant of the hepatobiliary cholesterol transporter (ABCG8 p.D19H) as the first common genetic risk factor for gallstone formation in humans.
Diagnostic Criteria and Clinical Characteristics
Presence of a colicky postprandial pain localized in epigastrium or in the right upper abdomen, in some patients accompanied by nausea or emesis.
Detection of gallbladder or common bile duct stones by
Abdominal ultrasonography (US)
Magnetic resonance cholangiopancreatography (MRCP)
Endoscopic retrograde cholangiopancreatography (ERCP)
Endoscopic ultrasonography (EUS)
Diagnostic evaluation should include at least one of the following (algorithm, Fig. 76-1):
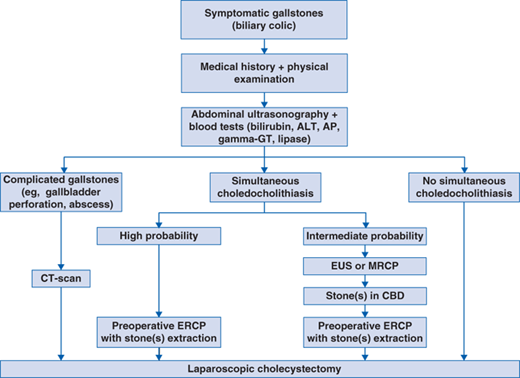
Detection of gallstones in asymptomatic patients without signs of complications does not necessitate further evaluation.
In symptomatic patients diagnostic evaluation should include
Blood tests including bilirubin, gamma-GT, alkaline phosphatase, alanine aminotransferase, lipase, and complete blood count.
Abdominal ultrasound to confirm or exclude presence of gallstones and their complications.
MRCP or EUS in patients with moderate probability of choledocholithiasis.
ERCP in case of common bile duct stones.
Abdominal CT scans in case of complications.
Individuals carrying gallstones can present with symptomatic and asymptomatic disease.
Symptoms of gallstones can be nonspecific.
Typical symptoms include colicky pain in the right upper quadrant, often radiating into upper back, lasting from at least 15 minutes to 5 hours.
Acute cholecystitis should be suspected in case of colicky pain lasting for more than 5 hours, positive Murphy sign (ie, tenderness above the gallbladder), fever, leukocytosis, and the following ultrasonographic features: thickening of the gallbladder wall (>3 mm), stratification of gallbladder wall into three layers, and fluid around gallbladder.
Cholangitis should be diagnosed in case of jaundice, fever, and/or right upper quadrant abdominal pain (the so-called Charcot triad).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


