Key Points
Disease summary:
The hemophilia A and B are sex-linked disorders leading to deficiencies of coagulation factor VIII (FVIII) and FIX, respectively. Bleeding is the hallmark of the disease, principally joint and soft tissue bleeding. The level of factor is directly related to the clinical severity of the disease where severe disease is less than 1% activity, moderate disease is 1% to 5%, and mild disease is greater than 5%. FXI deficiency (also known as hemophilia C), bleeding classically is not directly related to factor level and occurs several days after initial trauma or surgery. Antibodies to factor proteins termed inhibitors occur in 20% to 30% of FVIII patients and 2% to 4% of FIX patients. Inhibitor levels greater than 5 Bethesda units (BUI) require the use of bypassing agents such as Novoseven (FVIIa) and/or FVIII inhibitor bypassing activity (FEIBA).
Differential diagnosis:
Bleeding disorders such as von Willebrand disease, disseminated intravascular coagulopathy (DIC), liver disease, and acquired hemophilia may manifest clinically in a similar fashion.
Monogenic forms:
See above.
Family history:
30% of sex-linked disorders occur de novo, however, family history of hemophilia and inhibitor is important.
Twin studies:
Approximately 88% concordance rate of phenotype and inhibitor risk.
Environmental factors:
Involved with development of inhibitor such as time of factor infusion with coexisting inflammatory insult, high frequency of factor (time of surgery).
Genome-wide associations:
Modifier genes may affect predisposition for inhibitor development.
Pharmacogenomics:
The half-lives of FVIII and FIX are 12 and 20 hours, respectively. Intravenous infusions of recombinant or plasma-purified factors are the standard of care. New long-acting factors are in phase II or III of clinical trials.
Diagnostic Criteria and Clinical Characteristics
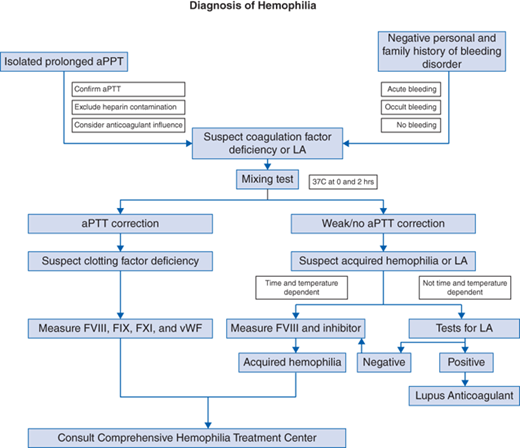
Diagnostic evaluation should include at least one of the following (see Fig. 32-1 algorithm):
Bleeding phenotype
Prolonged partial thromboplastin time (PTT) with normal prothrombin time (PT), normal platelet count
FVIII or FIX levels measured lower than normal (normal range 50%-150%)
FVIII and FIX inhibitor levels measured (normal <0.6 BUI)
Gold standard—mutational analysis of FVIII and FIX genes
Joint bleeding (spontaneous), muscle bleeding (spontaneous), epistaxis or gum bleeding, intracranial/subdural/epidural/subarachnoid bleeding, hematuria; circumcision bleeding



