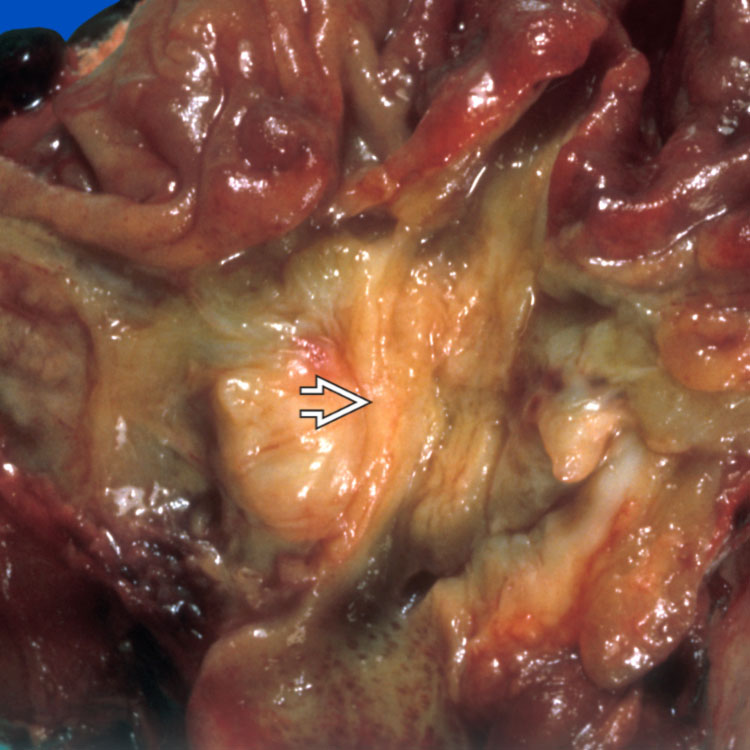
Pancreatic Ductal Adenocarcinoma A large pancreatic mass is encroaching on the duodenum with the ampulla of Vater overlying the mass .
Pancreatic Ductal Adenocarcinoma The cut surface is white, suggesting intense fibrosis. A few little cysts are evident within the mass . The dilated pancreatic duct is evident .
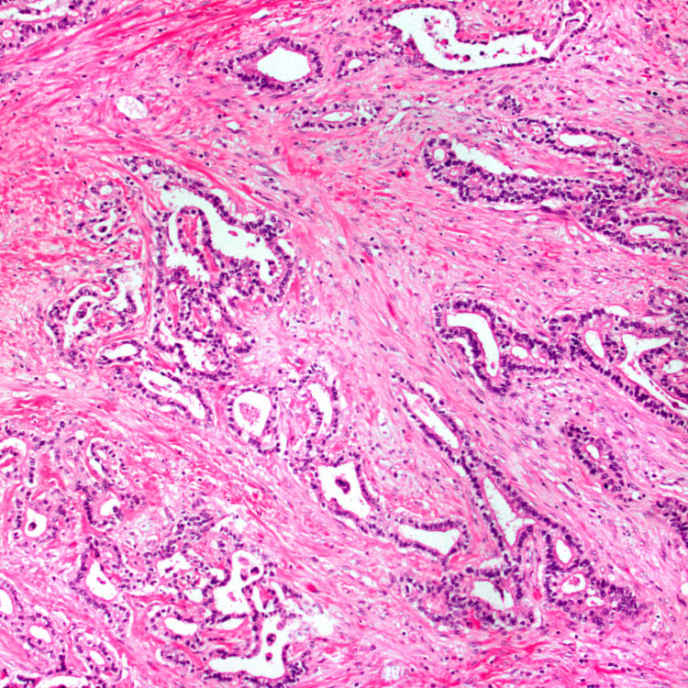
Well-Differentiated Adenocarcinoma This image shows small to medium-sized glands with haphazard growth embedded in dense desmoplastic stroma. The latter feature is a typical characteristic of this tumor.
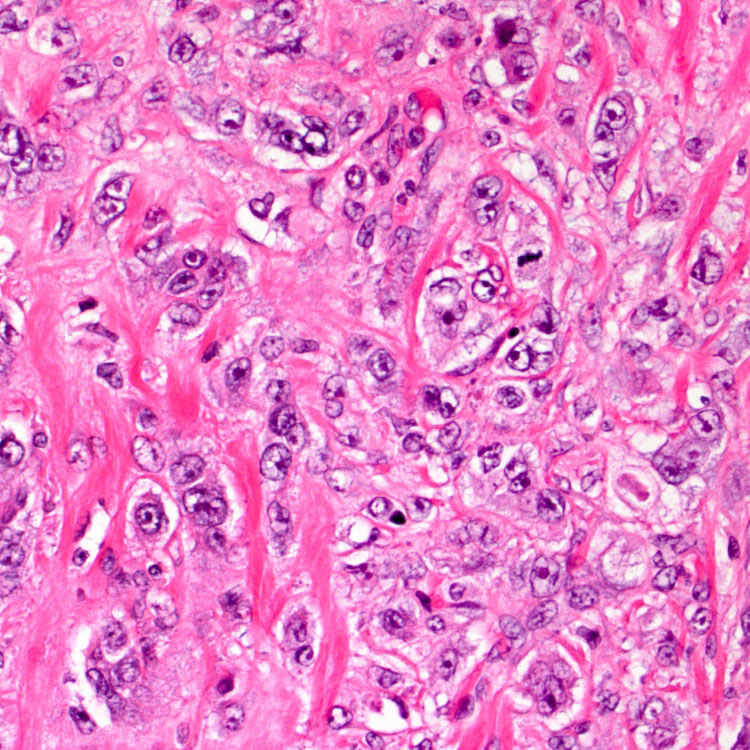
Poorly Differentiated Adenocarcinoma This image shows sheets of poorly differentiated tumor cells as well as single malignant cells. Heterogeneous morphology, encompassing well, moderate, and poor differentiations, is often seen in pancreatic ductal adenocarcinoma.
TERMINOLOGY
Abbreviations
• Pancreatic ductal adenocarcinoma (PDAC)
Synonyms
• Pancreatic adenocarcinoma
• Duct cell adenocarcinoma
Definitions
• Malignant epithelial neoplasm arising in pancreatic ductal system





 .
.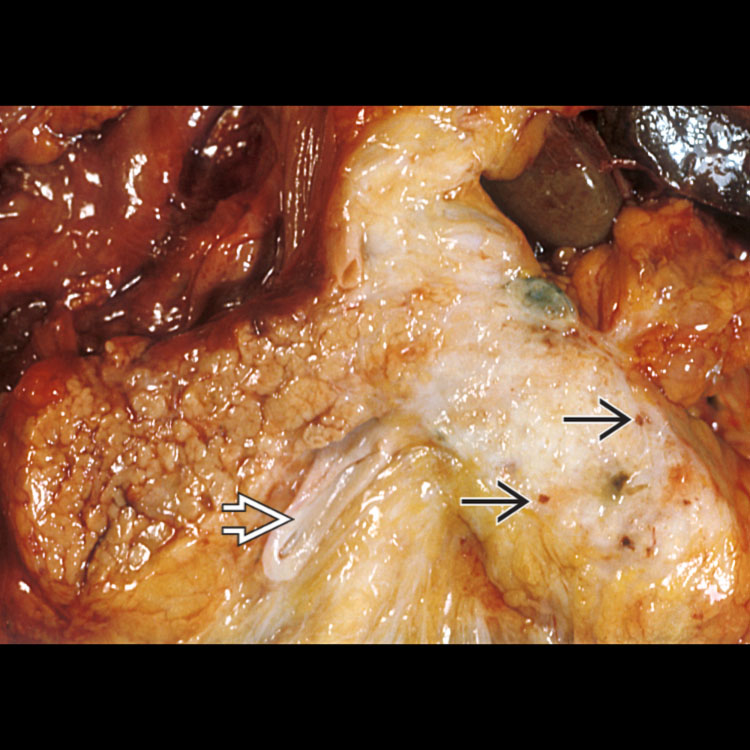
 . The dilated pancreatic duct is evident
. The dilated pancreatic duct is evident  .
.