Patient Story
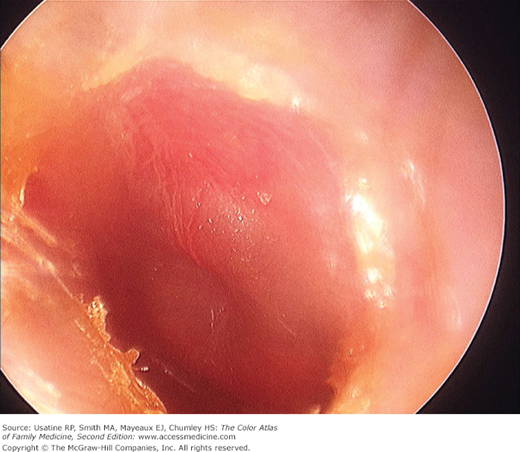
A 15-month-old boy is brought by both parents to his family physician with a 2-day history of fever, irritability, and frequent tugging of his left ear. This was preceded by a 1-week history of nasal congestion, cough, and rhinorrhea. On otoscopy, his left tympanic membrane (TM) appears erythematous, cloudy, bulging, and exudative (Figure 26-1). His left TM fails to move on pneumatic otoscopy. The physician diagnoses acute otitis media and decides with the parents to prescribe a 10-day course of amoxicillin; the child recovers uneventfully.
In follow-up 2 months later, the child appears healthy and is meeting all his developmental milestones. On otoscopic examination, air-fluid levels are seen in the right ear (Figure 26-2). The physician explains the diagnosis of otitis media with effusion to the parents and arranges follow-up. Three months later the effusion is completely resolved.

Introduction
Acute otitis media (AOM) is the most common diagnosis for acute office visits for children.1 AOM is characterized by middle-ear effusion in a patient with signs and symptoms of acute illness (e.g., fever, irritability, otalgia). Otitis media with effusion (OME) is a disorder characterized by fluid in the middle ear in a patient without signs and symptoms of acute ear infection; it is also very common in childhood.
Epidemiology
- AOM accounted for $5 billion of the total national health expenditure in 2000; more than 40% was incurred for children between 1 and 3 years of age.1
- It is estimated that 60% to 80% of children in the United States develop AOM by 1 year of age and that 80% to 90% develop AOM by 2 to 3 years of age.2,3
- The highest incidence occurs between 6 and 24 months of age.2,3
- AOM is the most common reason for outpatient antibiotic treatment in the United States.4 A national survey in 1992 revealed that 30% of all antibiotics prescribed for children younger than age 18 years was for treatment of AOM.5
- OME is diagnosed in 2.2 million children yearly in the United States.6
- Approximately 90% of children (80% of individual ears) have OME at some time before school age, most often between ages 6 months and 4 years.6
- The combined direct and indirect health care costs of OME amount to $4 billion annually.6
Etiology and Pathophysiology
- Pathogenesis of AOM includes:7
- Eustachian tube dysfunction (usually a result of an upper respiratory infection) and subsequent tube obstruction.
- Increased negative pressure in the middle ear.
- Accumulation of middle-ear fluid.
- Microbial growth.
- Suppuration (that leads to clinical signs of AOM).
- Eustachian tube dysfunction (usually a result of an upper respiratory infection) and subsequent tube obstruction.
- Most common pathogens in the United States and United Kingdom are:8,9
- Strains of Streptococcus pneumoniae not in the heptavalent pneumococcal vaccine (PCV7) (after introduction of PCV7 vaccine in 2000).
- Nonencapsulated (nontypable) Haemophilus influenzae (NTHi).
- Moraxella catarrhalis.
- Staphylococcus aureus.
- Strains of Streptococcus pneumoniae not in the heptavalent pneumococcal vaccine (PCV7) (after introduction of PCV7 vaccine in 2000).
- Viruses account for 16% of cases. Respiratory syncytial viruses, rhinoviruses, influenza viruses, and adenoviruses have been the most common isolated viruses.10
- Fluid limits sound conduction through the ossicles and results in decreased hearing.
- Reasons for the persistence of fluid in otitis media remain unclear, although potential etiologies include allergies, biofilm, and physiologic features.
- “Glue ear” refers to extremely viscous mucoid material within the middle ear and is a distinct subtype of OME.
Risk Factors
- The most important risk factors for AOM include young age and attendance at daycare centers.
- Other risk factors include:11
- White race.
- Male gender.
- History of enlarged adenoids, tonsillitis, or asthma.
- Multiple previous episodes.
- Bottle feeding.
- History of ear infections in parents or siblings.
- Use of a soother or pacifier.
- White race.
- Second-hand smoke is a risk factor when parents smoke at home.
- Risk factors for OME include age 6 years or younger, large number of siblings, low socioeconomic group, frequent upper respiratory tract infection, tobacco exposure, daycare attendance, and bottle feeding.12
Diagnosis
- To diagnose AOM, the clinician should confirm a history of acute onset, identify signs of middle-ear effusion (MEE), and evaluate for the presence of signs and symptoms of middle-ear inflammation.6 SOR C
- Elements of the definition of AOM are all of the following:6
Recent, usually abrupt, onset of signs and symptoms of middle-ear inflammation and MEE.
The presence of MEE. Although MEE is often presumed by bulging of the TM (Figure 26-1) or air-fluid level behind the TM (Figure 26-2), the guideline stresses use of objective measures of confirming MEE such as:6
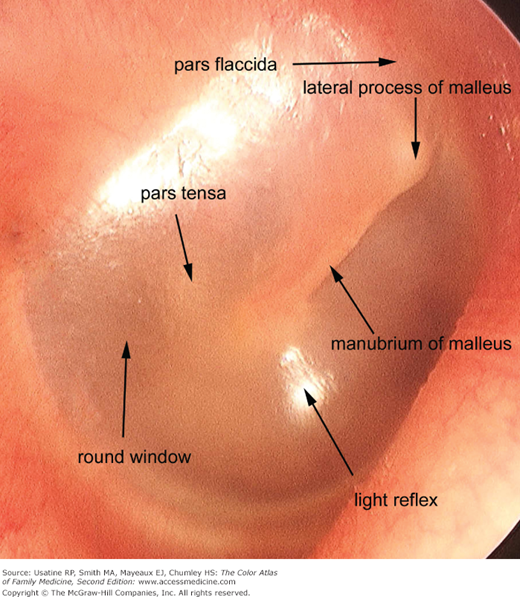
Limited or absent mobility of the TM established by pneumatic otoscopy—The TM does not move during air insufflation; often initially seen as retraction of the TM (Figures 26-3 and 26-4).
Objective measures such as tympanometry.
Otorrhea.
Signs or symptoms of middle-ear inflammation as indicated by either:
Distinct erythema of the TM (Figure 26-1) in contrast to the normal TM (Figure 26-5), or
Distinct otalgia (discomfort clearly referable to the ear[s] that results in interference with or precludes normal activity or sleep).

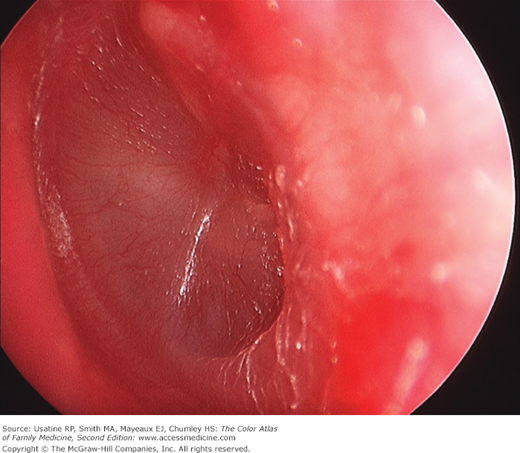
Figure 26-5

Acute otitis media, stage of suppuration. Note presence of purulent exudate behind the TM, the outward bulging of the TM, prominence of the posterosuperior portion of the drum, and generalized TM edema. The white area is tympanosclerosis from a previous infection. (Courtesy of William Clark, MD.)
- The most common symptom, present in more than half of patients, is mild hearing loss. This is usually identified when parents express concern regarding their child’s behavior, performance at school, or language development.12
- Absence of signs and symptoms of acute illness assists in differentiating OME from AOM.
- Common otoscopic findings include:
- Air-fluid level or bubble (Figure 26-2).
- Cloudy TM (Figures 26-4 and 26-6) in contrast to the normal TM (Figure 26-5).
- Redness of the TM may be present in approximately 5% of ears with OME.
- Air-fluid level or bubble (Figure 26-2).
- Clinicians should use pneumatic otoscopy as the primary diagnostic method for OME SOR A.13
- Impaired mobility of the TM is the hallmark of MEE.
- According to a metaanalysis, impaired mobility on pneumatic otoscopy has a pooled sensitivity of 94% and specificity of 80%, and positive likelihood ratio of 4.7 and negative likelihood ratio of 0.075.13
- Impaired mobility of the TM is the hallmark of MEE.
- Because AOM and OME are clinical diagnoses, diagnostic testing has a limited role. When clinical presentation and physical examination (including otoscopy) do not establish the diagnosis, the following can be used as adjunctive techniques:
- Tympanometry—This procedure records compliance of the TM by measuring reflected sound. AOM and OME will plot as a reduced or flat waveform. This technique requires patient cooperation but provides more objective data.
- Acoustic reflectometry—This procedure, very similar to tympanometry, measures sound reflectivity from the middle ear. With this test, the clinician is able to distinguish air- or fluid-filled space without requiring an airtight seal of the ear canal.
- Middle ear aspiration—For patients with AOM, aspiration may be warranted if patient is toxic, is immunocompromised, or has failed prior courses of antibiotics.
- Tympanometry—This procedure records compliance of the TM by measuring reflected sound. AOM and OME will plot as a reduced or flat waveform. This technique requires patient cooperation but provides more objective data.
Differential Diagnosis
The key differentiating feature between AOM and OME is the absence of signs and symptoms of acute illness in OME (e.g., fever, irritability, otalgia). Otoscopic findings may be similar. Other clinical entities that may be confused with AOM and OME include:
- Otitis externa—Otitis externa presents with otalgia, otorrhea and mild hearing loss, all of which can be present in AOM. Tragal pain on physical exam and signs of external canal inflammation on otoscopic exam differentiate it from AOM. Careful ear irrigation if tolerated may be helpful to visualize the TM to differentiate otitis externa from AOM (see Chapter 27, Otitis Externa).
- Otitic barotrauma—This often presents with severe otalgia. Key historical features include recent air travel, scuba diving, or ear trauma, preceded by an upper respiratory infection.
- Cholesteatoma—Unlike AOM, this is a clinically silent disease in its initial stages. Presence of white keratin debris in the middle ear cavity (on otoscopy) is diagnostic (Figures 26-7 and 26-8).
- Foreign body—A foreign body may present with otalgia. Otoscopy reveals presence of foreign body (see Chapter 28, Ear: Foreign Body).
- Bullous myringitis—Bullous myringitis is often associated with viral or mycoplasma infection as well as usual AOM pathogens; in approximately one-third of patients, there is a component of sensorineural hearing loss. Otoscopy shows serous-filled bulla on the surface of the TM (Figure 26-9

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


