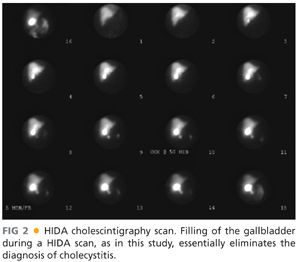
■ In atypical cases, a hepatobiliary iminodiacetic acid (HIDA) cholescintigraphy scan may be used to demonstrate obstruction of the cystic duct, which definitively diagnoses cholecystitis. Filling of the gallbladder during a HIDA scan essentially eliminates the diagnosis of cholecystitis (FIG 2).
■ HIDA scan is the diagnostic tool of choice in biliary dyskinesia and is performed with the concurrent administration of cholecystokinin. An ejection fraction of less than 20% is suggestive of the disease.
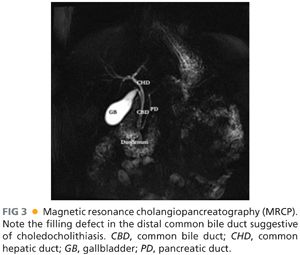
■ If there is suspicion of choledocholithiasis, as in patients with jaundice, pancreatitis, cholangitis, or dilated common bile duct on ultrasonography, the biliary tree can be delineated and inspected for presence of gallstones with the use of magnetic resonance cholangiopancreatography (MRCP) (FIG 3). MRCP is highly sensitive (>90%) and almost has a 100% specificity. As a noninvasive test, MRCP provides accurate imaging of the biliary tree, but in the setting of choledocholithiasis, it does not provide a therapeutic solution.
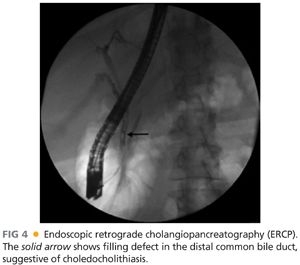
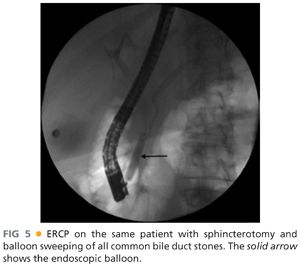
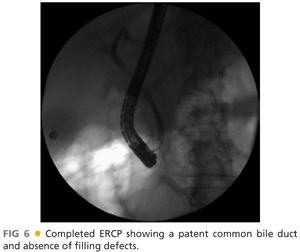
■ Endoscopic retrograde cholangiopancreatography (ERCP) can be used as a diagnostic and therapeutic modality (FIG 4). In the presence of stones in the common bile duct during ERCP, a sphincterotomy is performed to allow enlargement of the papilla and subsequent extraction of stones with a balloon or basket (FIGS 5 and 6). With this approach, more than 80% of all stones can be removed successfully. Larger stones may require additional removal techniques such as mechanical or intraductal lithotripsy. ERCP has a complication rate of around 8%; complications are sedation-related, pancreatitis, bleeding, perforation, and infection.
■ Preoperative laboratory studies should include liver function, renal function, electrolyte, and coagulation studies. Abnormal liver function studies may reflect choledocholithiasis or primary hepatic dysfunction.
SURGICAL MANAGEMENT
Preoperative Planning
■ In the preoperative area, the patient is asked if any conditions exist that were not present during the last clinic visit and would factor in the operative decision making; for example, a recent myocardial infarction or other cerebrovascular event.
■ The patient is asked to void just prior to transfer to the operating room so as to avoid placement of a Foley catheter that is not indicated for an elective laparoscopic cholecystectomy.
■ The operative consent, imaging, and laboratory values are reviewed.
Positioning
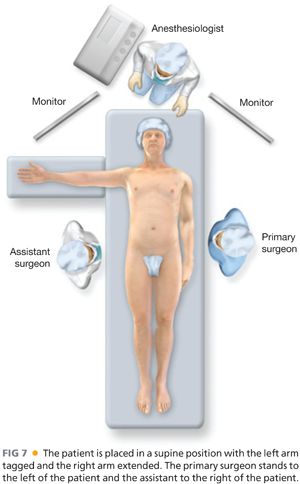
■ The patient is placed in a supine position with the right arm extended and the left arm is secured along the patient’s torso (FIG 7).
■ A footboard is placed at the patient’s feet, and the patient is strapped at the thighs and the legs to avoid a fall from the bed during steep reverse Trendelenburg position (FIG 8).

■ Heel pads, sequential compression devices for deep venous thrombosis prophylaxis, and warming devices are also placed.
■ An orogastric tube is inserted to decompress the stomach.
■ The primary surgeon stands at the patient’s left and the assistant surgeon at the patient’s right (FIG 7).
■ Two monitors are placed at the head of the bed, one on the right and one on the left, facing the surgeon and the assistant.
■ The laparoscopic camera, light source, insufflation tubing, suction, and electrocautery are passed to a tower at the feet of the patient.
TECHNIQUES
ENTRY INTO THE PERITONEAL CAVITY AND ACHIEVING PNEUMOPERITONEUM
■ The base of the umbilicus is grasped with two penetrating towel clips and is elevated for easier access. A 5-mm incision is created at the base of the umbilicus with the use of a no. 11 blade. The base of the umbilicus is chosen because it gives a better cosmetic result.
■ Through this incision, a Veress needle is introduced into the peritoneal cavity (FIG 9). A syringe with saline is attached to the Veress needle. First, aspirate the syringe to rule out placement of the Veress needle in the lumen of intestine or a vessel. Then infuse saline to determine if it will flow through the needle without resistance. This finding signifies that the needle is in the peritoneal cavity and not in the subcutaneous tissues. The insufflation tubing is attached to the Veress needle and pneumoperitoneum is achieved with 15 mmHg of CO2.

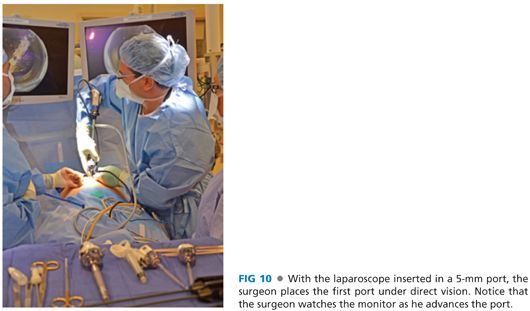
■ Next, a 0-degree laparoscope is inserted in a 5-mm OptiView port, and the port is inserted in the peritoneal cavity through the same incision under direct vision (FIG 10).
■ Alternatively, if the patient has a midline scar and a history of multiple intraabdominal procedures, entry into the peritoneal cavity is achieved through an incision in the left subcostal area just inferior to the rib in the anterior axillary line.
PLACEMENT OF THE OTHER PORTS
■ Once the first port is in place, inspect the intestines immediately beneath the incision to rule out any inadvertent injury. The 0-degree scope is replaced with a 30-degree scope that allows views through different angles.
■ The patient is then placed in reverse Trendelenburg position. The gallbladder is typically easy to visualize following this maneuver.
■ The next additional port to be placed is a 5-mm port in the patient’s right flank. The port is placed in the anterior axillary line around two fingerbreadths below the costal margin. Through this port, the assistant surgeon grasps the fundus of the gallbladder and retracts the gallbladder and the liver in an anterior and cephalad direction toward the diaphragm. This facilitates visualization of the triangle of Calot. If the gallbladder is very distended and inflamed, making it hard to be grasped, the gallbladder may be deflated with an endoscopic needle.
■ If the anatomy of the liver precludes visualization of the triangle of Calot, an additional 5-mm port is placed in the left anterior axillary line at the level of the costal margin and a liver retractor inserted.
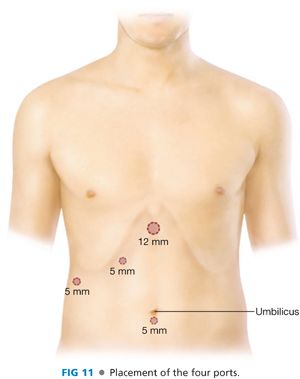
■ With this exposure, precise placement of the working port is determined. This is typically a 12-mm port that is placed in the epigastrium just below the xiphoid process and to the right of the falciform ligament. Ideally, the port is situated above the triangle of Calot just inferior to the liver edge.
■ The third port placed is a 5-mm port in the midclavicular line allowing for adequate spacing between the ports (FIG 11).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


