Incision
■ If the open J-tube placement is being done as a stand-alone operation, the incision should be centered in the midline at the level of the LOT.
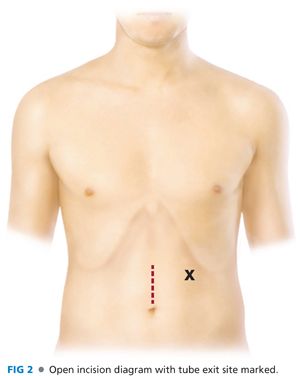
■ The supraumbilical vertical midline incision should be carried through the linea alba with enough length to locate the LOT, mobilize 20 to 30 cm of jejunum, and allow for fixation of the jejunal segment to the peritoneum of the abdominal wall around the tube exit site. If there are minimal adhesions, this incision may be kept relatively small, 5 to 7 cm, and the majority of the operation can be done on eviscerated jejunum (FIG 2).
■ A limitation of an incision that is too small is that it may prove difficult to fix the bowel to the abdominal wall through the small incision. Exposure of this step should not be compromised in anyway to avoid lengthening the incision.
Mobilization of Jejunum
■ Once the peritoneal cavity has been entered, the omentum and transverse colon are retracted cephalad to expose the small bowel. A segment of small bowel is chosen in the LUQ and traced proximally until the LOT is identified.
■ Once the LOT is identified, the small bowel is examined all the way to the ileocecal valve to ensure no occult pathology, obstruction, or torsion is present.
■ The tube insertion site is chosen where the tube will pass through the abdominal wall. This will generally be in the LUQ. The surgeon must ensure the chosen segment of jejunum will reach the parietal surface of the abdominal wall without any tension or torsion. Lysis of adhesions may be needed to make sure the jejunum can reach the abdominal wall without tension.
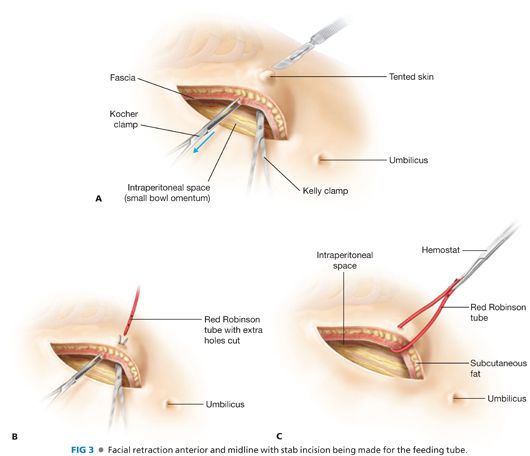
■ Placement of atraumatic clamps on the left side of the fascia allows the abdominal wall to be retracted anteriorly for exposure of tube placement. While keeping retraction, a strong fine clamp is passed from inside the abdomen through the point chosen in the abdominal wall. A 3-mm skin incision, at the clamp exit site, is created and the tube is grasped and the distal end is pulled through the abdominal wall into the peritoneal cavity. Both ends of the tube are clamped together and positioned out of the way (FIG 3).
Enterotomy and Placement of the Jejunostomy Tube
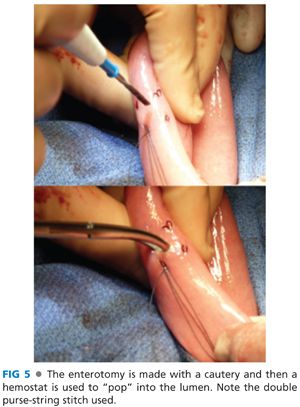
■ A segment of jejunum approximately 30 cm from the LOT is chosen as the site for the J-tube placement. This portion of jejunum can be eviscerated for the next steps if a smaller incision has been used. Using a 3-0 nonabsorbable or absorbable suture, place an approximately 4-mm purse-string suture in a box formation on the antimesenteric side of the small bowel (FIG 4). A double purse-string stitch may be used for additional security (FIG 5).

■ At this point, it is essential to note the proximal and distal ends of the jejunum and to ensure the orientation is maintained through the entire procedure.
■ Using cautery, create a small enterotomy in the center of the purse-string suture. It is helpful to grasp the bowel by the mesentery during this step. Inadvertent cautery injury to the opposite side of the small bowel can be avoided by cutting the serosa and muscularis with the cautery but “popping” into the lumen with a fine clamp (FIG 5).
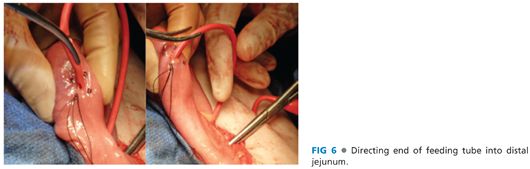
■ Place the distal end of the feeding tube through the enterotomy into the lumen and direct it distally. The catheter is advanced until at least 10 cm is intraluminal. It can be advanced further if there is an excessive amount of tubing left externally (FIG 6).
■ Tie down the purse-string suture, taking care not to overtighten and occlude the tube (FIG 7).

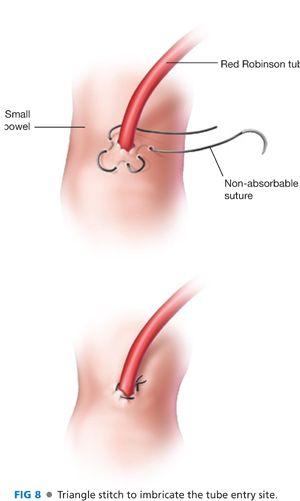
■ The tube entry sight is then imbricated using a three-point triangular technique (FIG 8).
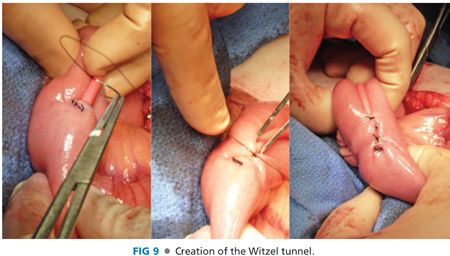
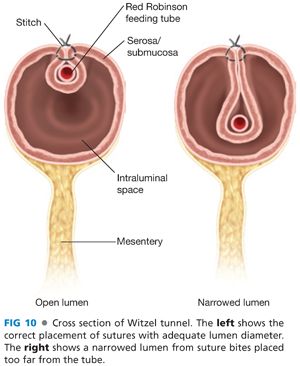
■ Next, a Witzel tunnel is created. Starting at the enterotomy, the small bowel is imbricated over the feeding tube using interrupted 3-0 absorbable suture on a taper needle (FIG 9) for a distance of about 5 cm. These are seromuscular bites spaced approximately 5 to 10 mm apart, ensuring the tube is not exposed. Care should be taken not to place the bites too far from the tube, as this will draw more bowel into the Witzel tunnel and narrow the jejunal lumen (FIG 10).
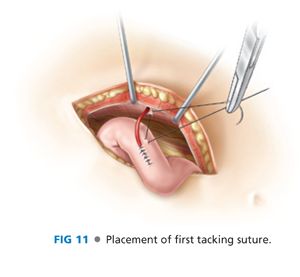
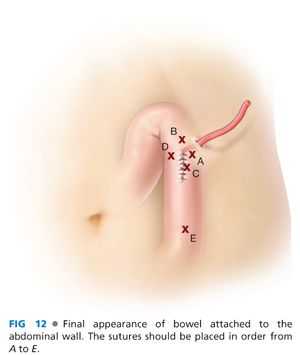
■ The jejunal segment must now be secured to the parietal peritoneum. This will allow the formation of a tract so that if the tube is inadvertently removed, it can be replaced without reentering the abdomen. This should be done in a way that the bowel is flush with the abdominal wall. Four “tacking” sutures of absorbable 3-0 suture can be placed around the tube exit site. The first is placed lateral to the tube, away from the operating surgeon. A seromuscular bite is taken and then a bite of peritoneum is taken at the corresponding location in the abdominal wall (FIG 11). Start with the lateral (furthest) suture first, then superior, inferior, and finally medial. Secure each suture with a clamp after it is placed and do not tie until they are all appropriately placed.
■ Once all four sutures have been placed, it is best to tie them in the order they were placed (FIG 12). An additional tacking suture may be placed 5 to 10 cm distally to secure a longer segment of bowel to the abdominal wall. This may help prevent torsion on the bowel around a single fixed point. The small bowel should now be adherent to the LUQ abdominal wall (FIG 13).
■ The external portion of the tube should be secured to the skin using a 2-0 nonabsorbable monofilament suture (FIG 14).

■ The abdomen is then closed in layers.
■ The tube may be capped or placed to gravity drainage via a bag. Covering the tube with a dressing and tape or abdominal binder will help prevent it from being inadvertently dislodged during patient movement.
LAPAROSCOPIC JEJUNOSTOMY
Equipment and Port Placement
■ Several commercially available laparoscopic jejunostomy kits are available. We use the Flexiflo Lap J™ laparoscopic jejunostomy kit by Abbott Nutrition. This section will describe J-tube placement using this kit. The steps described can be modified for other kits, and the package inserts for each kit should be read as they often contain pertinent pearls for success.
■ A standard laparoscopic setup including a 5-mm 0-degree or 30-degree laparoscope and two to three 5-mm ports is used.
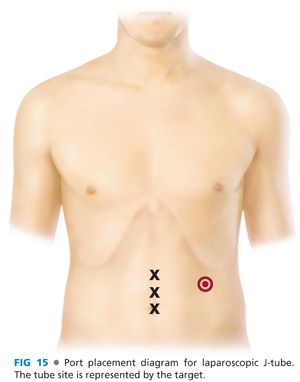
■ Port placement should triangulate toward the proposed tube exit site in the LUQ (FIG 15). The J-tube site should be at least two fingerbreadths below the left costal margin at approximately the midclavicular line.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


