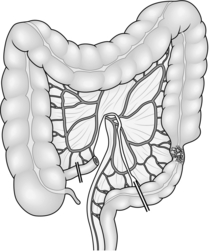
13 Preoperative assessment of the large bowel Laparoscopic right hemicolectomy Laparoscopic left hemicolectomy Anterior resection of the rectum Laparoscopic anterior resection Abdominoperineal excision of the rectum Colectomy for inflammatory bowel disease Elective colectomy and ileorectal anastomosis Elective total proctocolectomy 1. Obtain a full history and examine the abdomen, anus and rectum in every patient before undertaking surgery. Carry out further investigations as necessary: KEY POINTS Precautions 1. Perform a full laparotomy or laparoscopy, particularly if preoperative CT scanning has not been performed. 2. Examine the whole of the colon from the appendix to the rectum. Synchronous carcinomas occur in 4% of patients; adenomatous polyps cannot usually be palpated. 3. Avoid handling the carcinoma. Cover it with a swab soaked in 10% aqueous povidone-iodine solution. 4. Feel for enlarged lymph nodes in the mesentery and para-aortic region. Look and feel for liver and peritoneal metastases. 5. Assess the resectability and curability of the tumour. 6. If you discover unexpected liver metastases in the presence of a potentially resectable tumour do not biopsy them, as this may result in trans-peritoneal spread of tumour. In selected patients with solitary or localized liver metastases it may be appropriate to perform a synchronous metastasectomy if you have the relevant expertise. For multiple liver metastases the increased morbidity outweighs any benefit. Proceed with the planned bowel resection and refer the patient to a specialist liver centre for further assessment. 7. Curative resection should incorporate complete mesocolic excision (analogous to total mesorectal excision, vide infra). Excise the colon, segmental blood supply and associated lymph nodes en bloc within an intact mesocolic fascial envelope. If you fail to dissect in this plane you increase the risk of dissemination of tumour cells, resulting in local recurrence. 8. Treat carcinoma of the right colon by right hemicolectomy, taking the ileocolic pedicle at its origin from the superior mesenteric vessels (Fig. 13.1). For tumours of the hepatic flexure perform an extended resection, dividing the right branch of the middle colic pedicle at its origin (Fig. 13.2). If metastases are present perform a less radical resection without wide mesenteric clearance. Treat carcinoma of the transverse colon by extended right hemicolectomy or transverse colectomy (Fig. 13.3), mobilizing the hepatic and/or splenic flexure as required. 9. Treat carcinoma of the splenic flexure with left hemicolectomy, dividing the left colic pedicle at its origin (Fig. 13.4). If distal diverticular disease is present, perform an extended left hemicolectomy and swing the transverse and right colon down the right side of the abdomen to anastomose it to the rectum (Fig. 13.5). Alternatively, perform a subtotal colectomy and ileorectal anastomosis. 10. Treat carcinoma of the descending or sigmoid colon by left hemicolectomy, dividing the inferior mesenteric artery at its origin from the aorta and the inferior mesenteric vein at the same level (Fig. 13.6). 11. The surgical management of rectal carcinoma has undergone radical evolution over the last 20 years. Most cases of carcinoma of the rectum are now treated by restorative anterior resection using either a sutured, stapled or per-anal anastomosis. Abdominoperineal excision of the rectum and anus is required in around 20% of cases when it is impossible to obtain adequate distal clearance of the tumour. Carefully dissect in the pelvis to remove the mesorectum without breaching the fascial plane in which it is contained. Preserve the hypogastric nerve plexus if it is uninvolved with tumour, thereby reducing the incidence of erectile dysfunction and urinary complications. In expert hands total mesorectal excision (TME) results in very low local recurrence rates with an acceptable incidence of complications. 12. For high rectal carcinoma (tumours situated above the peritoneal reflection) with metastases, perform an anterior resection and primary anastomosis if you are able to perform this without the need for a defunctioning colostomy. These patients often have a limited survival and may never have the colostomy closed. For rectal carcinoma with unresectable local extension into the pelvic side wall, a Hartmann’s operation provides the best palliation. 1. Diverticular disease is common and elderly patients having abdominal surgery are often found to have diverticula, most commonly in the sigmoid colon. Although diverticular disease may be pancolonic, symptoms usually result from muscle hypertrophy causing thickening and shortening of the sigmoid colon. 2. Indications for elective resection are rarely absolute. Consider surgery in patients in good general health who have severe episodes of left iliac fossa and suprapubic pain with marked diverticular disease on a barium enema or CT scan and who are unresponsive to dietary change and antispasmodic drugs. More definite indications for surgical treatment include: 3. Colectomy for diverticular disease is frequently more challenging than similar operations for cancer. Even elective resections may be associated with pericolic inflammation, oedema and pericolic abscess formation in the mesentery. 4. It is unnecessary to remove all the proximal diverticula. Resect the hypertrophied section of bowel (usually the sigmoid colon), with anastomosis between the descending colon and the upper third of the rectum at or below the sacral promontory. 5. The elective treatment of choice is primary resection and anastomosis. If there is acute inflammation at the time of surgery or the anastomosis is difficult, perform a temporary defunctioning ileostomy. 1. Offer elective surgery to patients with persistent bloody diarrhoea, anaemia, weight loss and general ill-health who do not respond to treatment with corticosteroids and immune modulators such as azothiaprine. The majority of these patients havepancolitis (Greek: pan = all, total). Patients with distal disease involving the rectosigmoid or left hemicolon can usually be managed medically. Try to operate on patients during a remission. 2. Active colitis of 10 or more years’ duration may result in epithelial dysplasia with eventual progression to carcinoma, even in the absence of any symptoms. These patients require yearly surveillance with colonoscopy and mucosal biopsy. Advise operation if they develop severe dysplasia. Advise colectomy on any patient with total colitis and a stricture on barium enema or colonoscopy. Steroid therapy is not a contraindication to surgery, but steroid cover is required during and after the operation. 3. In longstanding total colitis, the colon is thickened, shortened and featureless in appearance. The macroscopic appearances may vary with parts of the colon appearing more actively inflamed with thickening, oedema and marked hyperaemia. The paracolic and mesenteric nodes may be enlarged. 4. The simplest operation is a proctocolectomy with a conventional end (Brooke) ileostomy, which removes all the inflamed bowel and potential cancer risk in one procedure. 5. Consider alternative procedures: 1. This can affect any part of the gastrointestinal tract from the mouth to the anus and is primarily treated medically. 2. Resort to surgery if medical treatment fails to control the disease, or for complications such as stricture causing obstructive symptoms, abscess or fistula formation. 3. All or part of the colon may be involved in Crohn’s disease. At laparotomy or laparoscopy carefully exclude disease in the stomach, duodenum and small bowel. Measure and record the sites and extent of disease and the length of residual small bowel following resection: patients with Crohn’s disease may require multiple operations and may develop short bowel syndrome if surgery is not carefully planned. 4. Crohn’s disease of the terminal ileum or ileocaecal region should be treated by ileocaecal resection, removing only the diseased segment: there is no advantage to removing macroscopically normal bowel. If there is a chronic abscess cavity in the right iliac fossa, position the anastomosis in the upper abdomen away from the inflamed tissues. 5. For extensive colitis unresponsive to medical treatment, perform a colectomy and ileorectal anastomosis or a total proctocolectomy and ileostomy. Stenosing or fistulating disease involving only the rectum may require abdominoperineal excision with an end colostomy. 6. Segmental colonic resection is appropriate for localized segmental involvement of the colon, or to treat internal fistula between the terminal ileum and the transverse or sigmoid colon. 1. Rectal polyps found at rigid sigmoidoscopy should be biopsied. If the polyp proves to be an adenoma, arrange a colonoscopy to find and remove any proximal polyps. Sessile villous adenomas usually occur in the rectum and can be removed by endoanal local excision. Transanal endoscopic microsurgery (TEMS) and endoscopic laser ablation (useful in the frail and elderly) are available in specialist centres. 2. If large colonic polyps are present in a patient undergoing surgery for carcinoma, extend the resection to include them or consider subtotal colectomy and ileorectal anastomosis. 3. Circumferential villous adenomas of the rectum are at high risk of malignant change and are difficult to resect peranally. Perform anterior resection with colo-anal anastomosis or a modified Soave procedure, particularly for tumours extending more than 10 cm from the anus. 4. Surgery is mandatory in familial adenomatous polyposis (FAP) to avoid inevitable malignant change. Options include colectomy and ileorectal anastomosis or proctocolectomy and ileoanal pouch reconstruction. Following ileorectal anastomosis the rectum still carries the potential for malignant change. Inspect sigmoidoscopically every 6–12 months with fulguration of polyps over 5 mm in diameter. 1. Urgent operations on the colon or rectum are required for obstruction, perforation, acute fulminant colitis and, less frequently, life-threatening acute haemorrhage. 2. Stabilize the patient’s condition prior to surgery by replacing blood, fluid and electrolyte losses. Give broad-spectrum antibiotics (co-amoxiclav or a cephalosporin with metronidazole) to counteract sepsis. 3. Major abdominal sepsis, perforation or torrential haemorrhage demand operation as soon as the patient’s condition allows. Patients with colonic obstruction or inflammatory bowel disease rarely require immediate surgery and frequently benefit from appropriate investigation and resuscitation. 1. Establish the site of obstruction with a CT scan or water-soluble contrast enema. 2. If the patient is unfit for surgery, a stenosing tumour may be suitable for radiological stenting to open up the bowel lumen, allowing the patient’s condition to be optimized for subsequent elective surgery. Stenting is less successful for benign strictures due to diverticulitis, Crohn’s disease or external compression and carries a higher morbidity: a defunctioning proximal stoma provides better palliation in patients who are unfit for major surgery. 3. Urgent resection should be as radical as would be achieved electively, provided the patient’s condition permits this. If metastases are present, undertake a less radical resection if possible, as this will give better palliation. 4. Perform a right hemicolectomy for carcinoma of the right colon causing acute intestinal obstruction. It is rare to find a proximal tumour that is not resectable. Avoid a bypass operation if possible as this may relieve the obstruction but it will not stop bleeding from the tumour and consequent anaemia, nor will it palliate pain or complications resulting from invasion of other structures. 5. Historically, left-sided obstruction was treated by a three-stage procedure with an initial proximal stoma to relieve the obstruction, subsequent resection and anastomosis and, when the anastomosis was healed, closure of the stoma. Obstructing carcinoma of the sigmoid or descending colon is now usually treated by a one-stage colectomy with ileosigmoid or ileorectal anastomosis (Fig. 13.7). If a left-sided tumour is unresectable, create a proximal defunctioning colostomy. 6. Treat carcinoma of the rectosigmoid junction or rectum by resection and primary anastomosis with or without a defunctioning ileostomy. Alternatively, perform a Hartmann’s procedure (vide infra). 7. Acute obstruction due to diverticular disease is often complicated by paracolic abscess formation, and is most commonly treated by Hartmann’s procedure. However, if the infection is localized and can be completely excised then primary resection and anastomosis, with or without a defunctioning ileostomy, may be appropriate. 1. Perforation of a carcinoma or diverticular disease requires resection and anastomosis with a covering stoma; if major faecal contamination is present, perform a Hartmann’s procedure. 2. If CT scanning demonstrates a localized perforation and pericolic abscess, drain it percutaneously. Operate if initially localized abdominal signs become more generalized or if the infection fails to settle despite adequate conservative therapy. Generalized purulent peritonitis secondary to diverticulitis may be managed by laparoscopic peritoneal lavage and drainage, provided there is no evidence of a free perforation. In patients with more extensive contamination and a free perforation, resection and primary anastomosis is possible in selected cases, but do not perform this in the presence of faecal peritonitis. 3. Primary anastomosis is increasingly popular because: 4. Always aim to resect the perforated segment of bowel, even in an acutely ill patient, to minimize the risk of persistent contamination. Also, it is difficult at operation to decide whether a lesion is a perforated carcinoma or diverticular phlegmon: up to 25% of patients with a preoperative diagnosis of perforated diverticulitis will prove to have malignancy. If carcinoma is suspected perform a radical resection: examination of the resected specimen in theatre may help to confirm the diagnosis. 1. Treat acute fulminant colitis, with or without toxic megacolon, by colectomy and ileostomy. Do not excise the rectum. It is usually safe to close the rectal stump but if it is very inflamed or friable you may need to bring it out as a mucous fistula. Alternatively, close the stump directly under the wound so that if it breaks down it will not contaminate the peritoneal cavity. 2. In ischaemic colitis, excise the segment of acutely ischaemic colon and create a proximal (and if necessary a distal) colostomy. Do not remove the rectum or distal sigmoid colon as these usually recover sufficiently for an anastomosis to be carried out later. 1. If possible, determine the site of bleeding by sigmoidoscopy, colonoscopy, upper gastrointestinal endoscopy and angiography. In patients with episodes of haemorrhage and diverticular disease do not assume causation: 50% have another cause for the bleeding. 2. It is usually possible to arrest life-threatening bleeding by interventional radiology and embolization, which carries a much lower morbidity and mortality than emergency colectomy. Surgery may still be required if the embolized segment becomes ischaemic, but at least you will be sure which part to remove. 1. Morbidity and mortality following colonic surgery are higher than following small bowel resection. Infection is more common, resulting in abscess formation with potentiation of collagenase activity which predisposes to anastomotic dehiscence. 2. In addition, the colonic blood supply is more tenuous and tissue perfusion may be suboptimal postoperatively, resulting in ischaemia to the anastomosis. If available, we recommend goal-directed intra-operative fluid replacement using peroperative transoesophageal Doppler monitoring. 1. Enhanced recovery protocols (‘fast track surgery’) have demonstrated reduction in both morbidity and length of stay following elective colorectal resections. They typically include: 2. There is no evidence to support the routine use of bowel preparation before elective colonic operations and good evidence that the resulting fluid and electrolyte imbalances delay postoperative recovery. Some surgeons nonetheless prefer to prepare the left colon, but there is no need to clear the bowel prior to right hemicolectomy. Always prepare the bowel prior to low anterior resection with a loop ileostomy, as this will otherwise leave a long segment of faecally loaded colon between the covering stoma and the anastomosis. Sodium picosulfate and magnesium citrate (Picolax™, Citrafleet™), sodium phosphate (Fleet™) and polyethylene glycol (Kleanprep™, Moviprep™) are all suitable. Encourage adequate oral fluids during bowel preparation: intravenous fluids may be required in elderly patients. Patients likely to have a transanal stapled anastomosis should have an enema prior to surgery to avoid the problem of a rectum loaded with stool. 3. Give preoperative prophylactic antibiotics at induction of anaesthesia: a cephalosporin or a broad-spectrum penicillin plus beta-lactamase inhibitor (co-amoxiclav) plus metronidazole are suitable. Give a second dose of antibiotics if the duration of operation is more than 2 hours or if there is significant intraoperative contamination. There is no evidence that routine use of more than one dose of prophylactic antibiotics reduces the risk of infection, unless gross faecal contamination is present, when antibiotics should be continued for several days postoperatively. 4. Catheterize the patient after induction of anaesthesia and monitor urinary output during and after surgery. 1. Clamp the segment of bowel to be resected with Parker-Kerr clamps or use a cross-stapling technique. Do not clamp the ends to be sutured: apply non-crushing clamps 5 cm away from the bowel end to avoid contamination while constructing the anastomosis. 2. A good blood supply is crucial to anastomotic healing. Ensure that both limbs of the anastomosis are pink and well perfused: visible or palpable pulsation in the mesenteric vessels is an added reassurance, as is pulsatile flow on dividing the marginal artery whilst preparing the bowel for anastomosis. 3. Divide the colon at right-angles to the mesentery. If there is disparity in size between the ends, particularly when carrying out a right hemicolectomy or an ileorectal anastomosis, make a slit in the antimesenteric border of the ileum until the two ends approximate in size. Alternatively, carry out a stapled side-to-side anastomosis. When anastomosing a long proximal limb of mobilized colon to the rectum check that it is not twisted through 360°. Clean the ends of the bowel to be sutured with swabs moistened in aqueous 10% povidone-iodine solution. 4. Suture the bowel using a single-layer seromuscular suture such as 3/0 PDS (polydioxanone sulphate) using either an interrupted or continuous technique. Invert the edges to ensure no mucosa protrudes from the suture line. Where the two bowel limbs are sufficiently mobile and well perfused a side-to-side stapled anastomosis is a quick and reliable technique, although significantly more expensive. This technique is ideally suited to small bowel and right colonic resections, but should be used with caution in the left colon where the blood supply is more tenuous. 5. Colorectal anastomosis is most easily accomplished using a circular stapling device such as the CEEA stapler, using a 28-or 31-mm diameter device. We particularly recommend it for anastomosis low in the pelvis where suturing may be technically difficult. 6. Prevent contamination of the operative field by placing a non-crushing clamp across the bowel 10 cm from the end before this is swabbed out and cleaned. Isolate the anastomosis from the peritoneum and wound edges while it is being constructed, using disposable drapes or abdominal packs soaked in 10% aqueous povidone-iodine solution. On completion of the anastomosis, discard any soiled packs and instruments and change gloves before closing the abdomen. 7. Intra-peritoneal drains are of no proven value and may actually increase the risk of anastomotic leakage. Some surgeons prefer to drain the pelvic cavity following low anterior resection or abdominoperineal excision. 1. The indications for laparoscopic colectomy are essentially the same as for open surgery. The laparoscopic approach is associated with some short-term benefits when compared with open surgery, notably faster recovery and reduced postoperative pain and wound infection. Data from randomized trials have demonstrated oncological outcomes comparable to open surgery. 2. Like other advanced laparoscopic procedures, laparoscopic colectomy is associated with a steep learning curve, requiring around 30 resections to achieve competence. Mobile lesions in the right colon or rectosigmoid junction are ideal for the novice. Lesions in the upper sigmoid or descending colon which necessitate splenic flexure mobilization and mid or low rectal tumours, which require pelvic dissection, require considerably more skill and experience. 3. Patient-related factors such as obesity and previous abdominal operations can make laparoscopic surgery more difficult, although conversely laparoscopic colectomy may result in greater short-term benefits in these patients. Patients with compromised cardiopulmonary function require special attention as they tolerate prolonged pneumoperitoneum poorly: close liaison with an experienced anaesthetist is recommended. Patients with locally advanced disease (tumours with fixation to surrounding structures or contiguous organ involvement) should be selected with extreme caution. Such tumours often preclude a pure laparoscopic approach (although you may employ a ‘hand-assisted’ laparoscopic approach with the use of hand-access devices) and are better managed through a conventional laparotomy incision. 4. As abdominal organs cannot be palpated during laparoscopy, preoperative colonoscopy and imaging studies are important both for tumour localization and disease staging. If preoperative colonoscopy is incomplete, either barium enema examination or CT virtual colonoscopy should be considered for proximal colonic evaluation; the latter also facilitates better patient selection by providing information on tumour staging. 5. ‘Tattoo’ small mucosal lesions during endoscopic examination to facilitate identification at subsequent laparoscopy. Alternatively, carry out perioperative colonoscopy, preferably with CO2 insufflation, during surgery. 6. Laparoscopic colectomy is never a single surgeon operation. Always use a dedicated team of at least two experienced surgeons and one camera assistant. Experienced anaesthetists, nurses and technicians who are familiar with the procedures, laparoscopic instruments and ancillary technology also form an integral part of the team. The operating theatre should accommodate staff and equipment in an unencumbered fashion. If possible, carry out laparoscopic colectomy in an integrated endo-laparoscopic operating suite where all equipment, including the optical system, energy source and monitors, is placed on ceiling-mounted platforms. Back-up equipment and facilities are essential. 7. Recommended instruments for laparoscopic colectomy: 1. Perform this operation for carcinoma of the caecum and ascending colon, benign tumours of the right colon, perforated caecal diverticulum, midgut neuroendocrine tumours and carcinoma of the appendix. Small, low-grade neuroendocrine tumours of the tip of the appendix (appendiceal carcinoid) found incidentally at appendicectomy do not require subsequent hemicolectomy. 2. In benign disease of the terminal ileum, particularly Crohn’s disease, resect the diseased ileum together with the caecum and 2–3 cm of the right colon. If ileocaecal Crohn’s disease is associated with abscess formation in the right iliac fossa, place the anastomosis in the upper abdomen away from the abscess cavity to reduce the risk of postoperative fistula formation. 3. Do not site a small bowel anastomosis close to the ileocaecal valve, as this may predispose to anastomotic leakage. It is preferable to remove the caecum and a small part of the ascending colon to achieve an ileocolic anastomosis. 4. In patients with distal colonic obstruction the caecum may be ischaemic: include any non-viable bowel in the resection, either by means of an extended right hemicolectomy or subtotal colectomy with ileorectal anastomosis. 1. Make a midline incision centred on the umbilicus or a transverse incision extending laterally from the umbilicus. Handle the tumour as little as possible. If the serosa is infiltrated by carcinoma, cover it with a swab soaked in aqueous 10% povidone-iodine solution. 2. Draw the caecum and ascending colon medially. Divide the parietal peritoneum in the lateral paracolic gutter from the caecum to the hepatic flexure. If the carcinoma infiltrates the lateral abdominal wall do not attempt to dissect it off, but excise a disc of peritoneum and underlying muscle en-bloc with the specimen. 3. Dissect the plane between the right colon and posterior abdominal wall, identifying and preserving the right gonadal vessels, ureter and duodenum. 4. Mobilize the hepatic flexure and posterior attachments of the terminal ileum so that the whole of the right colon can be lifted medially and out of the abdomen.
Colon
PREOPERATIVE ASSESSMENT OF THE LARGE BOWEL
 Rigid sigmoidoscopy. Although increasingly superseded by flexible sigmoidoscopy, this remains a useful investigation in outpatients presenting with bowel symptoms as it allows for prompt identification and biopsy of rectal pathology such as carcinoma, proctitis or solitary rectal ulcer.
Rigid sigmoidoscopy. Although increasingly superseded by flexible sigmoidoscopy, this remains a useful investigation in outpatients presenting with bowel symptoms as it allows for prompt identification and biopsy of rectal pathology such as carcinoma, proctitis or solitary rectal ulcer.
 Colonoscopy (see Chapter 12). This is the investigation of choice for the large bowel, although not without risks, especially in the elderly or during therapeutic procedures. Biopsies can be obtained from tumours and inflammatory bowel disease and pedunculated polyps can be removed by colonoscopic snaring. More advanced procedures, such as endoscopic submucosal resection and stenting, are available in many centres. The risk of perforation is approximately 1:800; removal of large polyps also carries a significant risk of bleeding although this can usually be controlled endoscopically.
Colonoscopy (see Chapter 12). This is the investigation of choice for the large bowel, although not without risks, especially in the elderly or during therapeutic procedures. Biopsies can be obtained from tumours and inflammatory bowel disease and pedunculated polyps can be removed by colonoscopic snaring. More advanced procedures, such as endoscopic submucosal resection and stenting, are available in many centres. The risk of perforation is approximately 1:800; removal of large polyps also carries a significant risk of bleeding although this can usually be controlled endoscopically.
ELECTIVE OPERATIONS
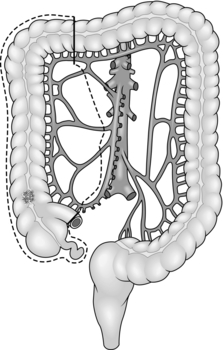
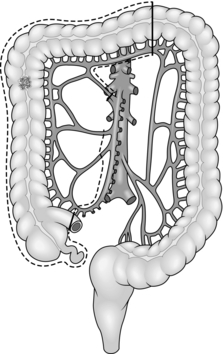
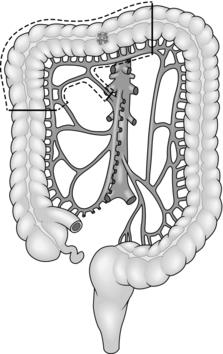
CARCINOMA
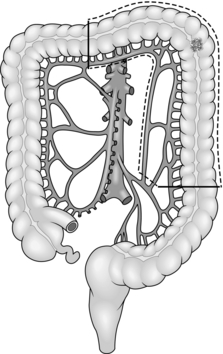
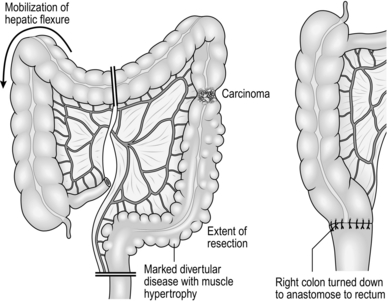
Assess
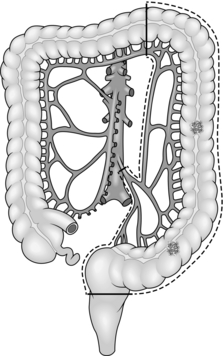
DIVERTICULAR DISEASE
 Younger male patients (less than 50 years of age) with symptomatic disease, since statistically over 80% eventually come to surgery, many with complications
Younger male patients (less than 50 years of age) with symptomatic disease, since statistically over 80% eventually come to surgery, many with complications
ULCERATIVE COLITIS
CROHN’S DISEASE
POLYPS AND POLYPOSIS
URGENT OPERATIONS
OBSTRUCTION
PERFORATION
 Patients require one operation rather than two
Patients require one operation rather than two
 Reversal of Hartmann’s procedure can be challenging, particularly if attempted too early.
Reversal of Hartmann’s procedure can be challenging, particularly if attempted too early.
ACUTE INFLAMMATORY OR ISCHAEMIC BOWEL DISEASE
ACUTE MASSIVE HAEMORRHAGE
PRINCIPLES OF COLECTOMY
Appraise
Prepare
 Avoidance of mechanical bowel preparation (vide infra)
Avoidance of mechanical bowel preparation (vide infra)
 The use of minimally invasive surgery or small incisions
The use of minimally invasive surgery or small incisions
 Goal-directed fluid replacement (vide supra)
Goal-directed fluid replacement (vide supra)
 Prevention of intra-operative hypothermia
Prevention of intra-operative hypothermia
 Avoidance or early removal of nasogastric tubes, drains and urinary catheters
Avoidance or early removal of nasogastric tubes, drains and urinary catheters
Action
LAPAROSCOPIC COLECTOMY
 Three to four atraumatic forceps for handling of bowel and fine tissues
Three to four atraumatic forceps for handling of bowel and fine tissues
 Two grasping forceps for holding sutures or cotton tapes
Two grasping forceps for holding sutures or cotton tapes
 Laparoscopic bipolar coagulating forceps (Gyrus Medical Limited, Cardiff, U.K.), 5 mm in size
Laparoscopic bipolar coagulating forceps (Gyrus Medical Limited, Cardiff, U.K.), 5 mm in size
 Endoscopic clip applicators and clips
Endoscopic clip applicators and clips
 Circular staplers for trans-rectal bowel anastomosis
Circular staplers for trans-rectal bowel anastomosis
 A sterile plastic zip-lock bag, used as a parietal protector during specimen retrieval.
A sterile plastic zip-lock bag, used as a parietal protector during specimen retrieval.
RIGHT HEMICOLECTOMY
Appraise
Action
Resect
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree