CASE 54
A 27-year-old woman was seen in a clinic for complaints of fevers, chills, headache, malaise, anorexia, and abdominal pain for several days. She stated she came today because she noticed that her eyes had turned yellow, and she had developed a very bothersome generalized itching.
LABORATORY STUDIES
Diagnostic Work-Up
Table 54-1 lists the likely causes of illness (differential diagnosis). For suspected viral hepatitis, serology is the mainstay of specific diagnosis. The hepatitis serology panel should include testing of hepatitis (A, B, and C) viral antigens and antibodies.
TABLE 54-1 Differential Diagnosis and Rationale for Inclusion (consideration)
Rationale: Hepatitis is a relatively common clinical syndrome associated with hepatocyte injury, jaundice, and elevation of liver enzymes (ALT and AST >500 IU/L). The major infectious causes of hepatitis are hepatitis viruses (HAV, HBV, or HCV), where elevation of ALT is more pronounced than AST. Alcoholic liver injury does not lead to ALT or AST levels >500 IU/L and AST is higher than ALT. The other listed agents may not cause such elevations of ALT and AST, but they can also occur with similar symptoms. Sometimes risk factors can shed light on one etiology over others. Liver abscess should be detected with abdominal imaging and is not usually associated with significant jaundice. Noninfectious etiologies should be ruled out. Drugs, particularly acetaminophen, can also cause such elevations in transaminases. Gallstone hepatitis may cause similar symptoms due to blockage of bile but may not show marked increase in liver enzymes. Infection with CMV and EBV can be associated with elevated liver enzymes but without significant jaundice.
MICROBIOLOGIC PROPERTIES
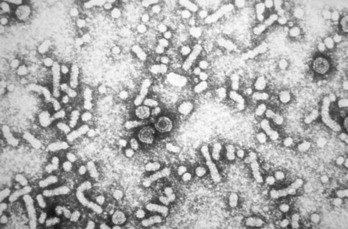
HBV is a 42-nm, double-shelled DNA virus (genus: Orthohepadnavirus; family: Hepadnaviridae). The genome is a 3.2-kb circular, double-stranded, incomplete DNA. The viremic patient’s blood may present three different particles under electron microscopy (Fig. 54-1). The larger (42-nm) rounded bodies are full assembly infectious virus particles with a lipid envelope. The two smaller particles are a spherical (27-nm) nucleocapsid core and tubular or filamentous (22-nm) particles of surface proteins (HbsAg). The envelope protein expressed on the outer surface of the full virion and on the smaller spherical and filamentous particles is called hepatitis B surface antigen (HBsAg). The smaller spherical and tubular structures carrying HBsAg are thought to be produced in blood for decoy functions and evasion of the immune system. HBsAg is the primary component of the hepatitis B vaccine; this antigen induces a protective, neutralizing antibody that provides long-term protection against HBV infection. The inner core of the virus contains hepatitis B core antigen (HBcAg), hepatitis Be antigen (HBeAg), a single molecule of partially double-stranded DNA, and DNA-dependent DNA polymerase (with reverse transcription function). The three antigens, HBsAg, HBcAg, and HBeAg, and the selected, specific antibodies, constitute hepatitis B diagnostic markers. HBV does not grow in cell cultures, but HBV DNA can transfect surrogate cells, producing viral proteins.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


